

Complete reperfusion is required for maximal benefits of mechanical thrombectomy in stroke patients
- PMID: 28912596
- PMCID: PMC5599658
- DOI: 10.1038/s41598-017-11946-y
Complete reperfusion is required for maximal benefits of mechanical thrombectomy in stroke patients
Abstract
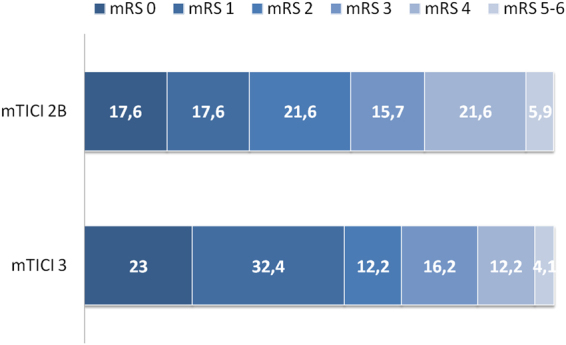
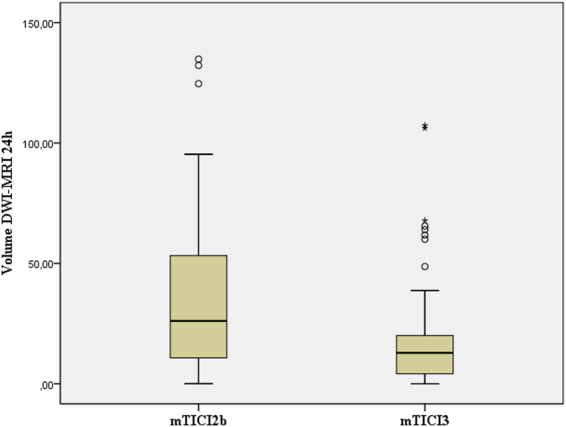
A mTICI 2b or a mTICI 3 score are currently considered success following mechanical thrombectomy (MT) in acute stroke but is undetermined whether the two scores translate equivalent outcomes. We present a single-center, retrospective cohort of patients with anterior circulation stroke treated with MT and achieving a final mTICI score 2b or 3. A multimodal CT at baseline and a multimodal MRI at 24 hours assessed the growth of the infarct, and the modified Rankin Scale (mRS) assessed functional outcome at 90 days. The primary outcome was the shift analysis of the mRS at day 90 in ordinal regression adjusted for covariates (age, sex, pretreatment NIHSS score, target occlusion, infarct core, pretreatment alteplase), and the collateral score. Infarct growth was explored in a similarly adjusted multiple linear regression model. MT was started within a median of 285 minutes of symptom onset; 51 (41%) patients achieved a mTICI 2b, and 74 (59%), a mTICI 3. mTICI 3 resulted in better mRS score transitions than mTICI 2b (odds ratio 2.018 [95% CI 1.033-3.945], p = 0. 040), and reduced infarct growth (p = 0.002). We conclude that in patients with acute stroke receiving MT, success should be redefined as achieving a mTICI 3 score.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
