

Orbital Floor Fracture
- PMID: 28913267
- PMCID: PMC5556798
- DOI: 10.7181/acfs.2016.17.3.111
Orbital Floor Fracture
Abstract
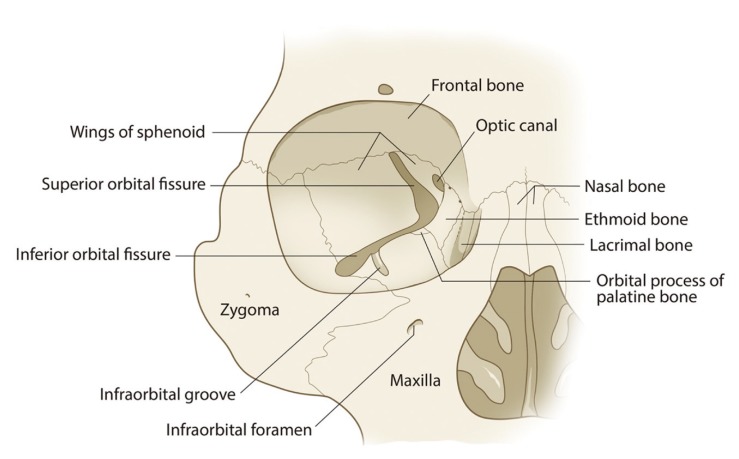
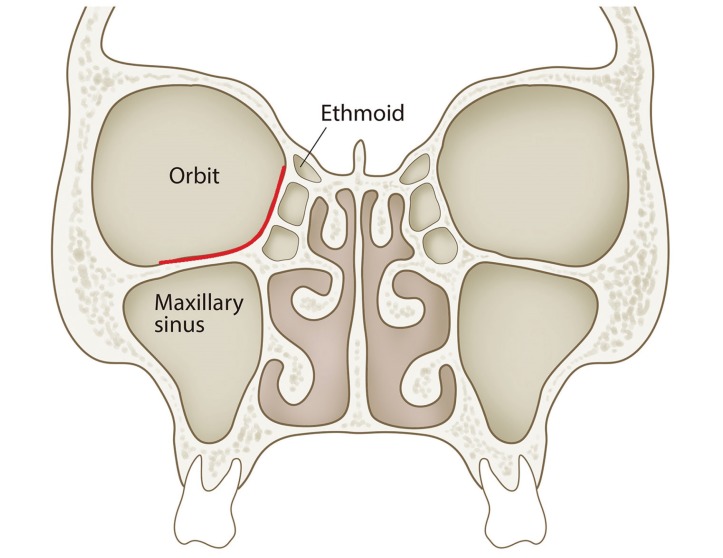
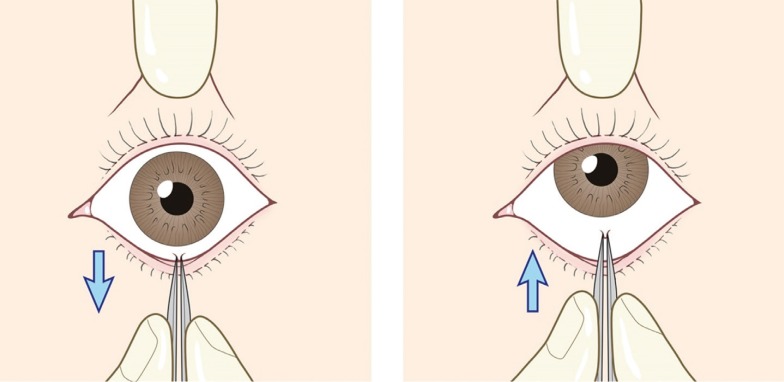
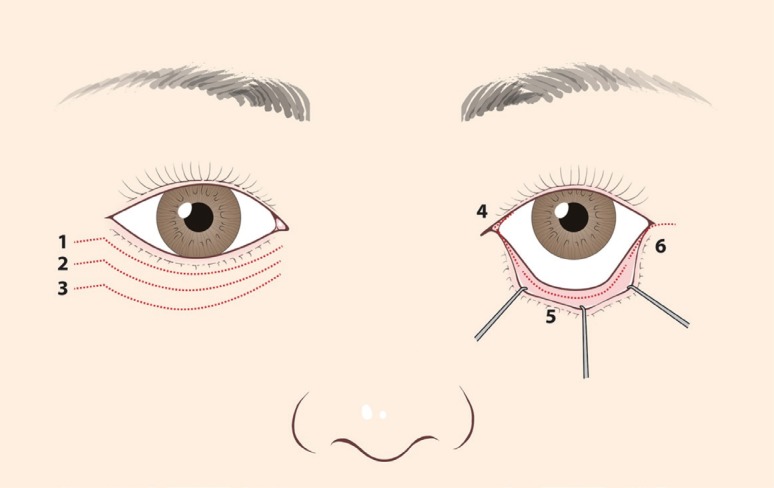
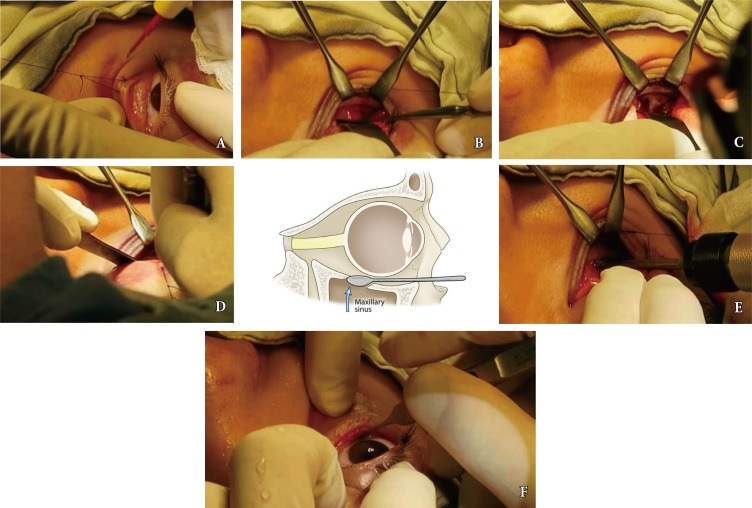
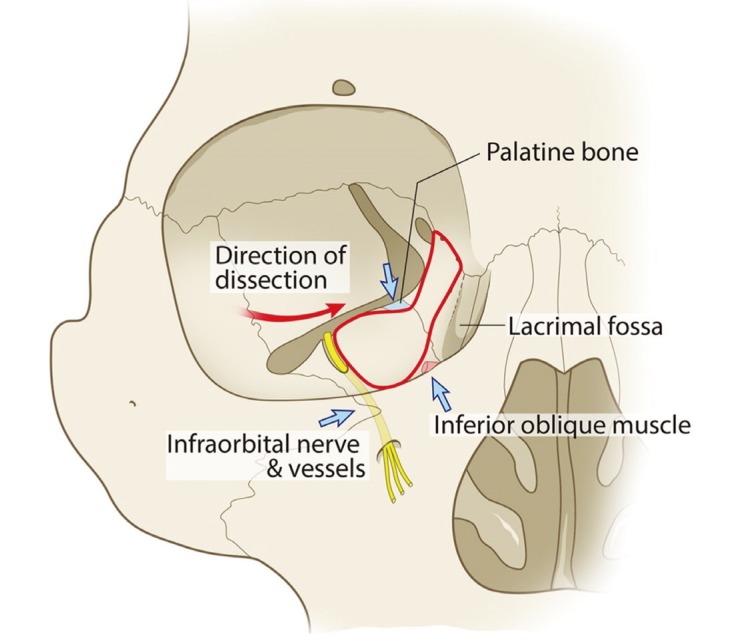
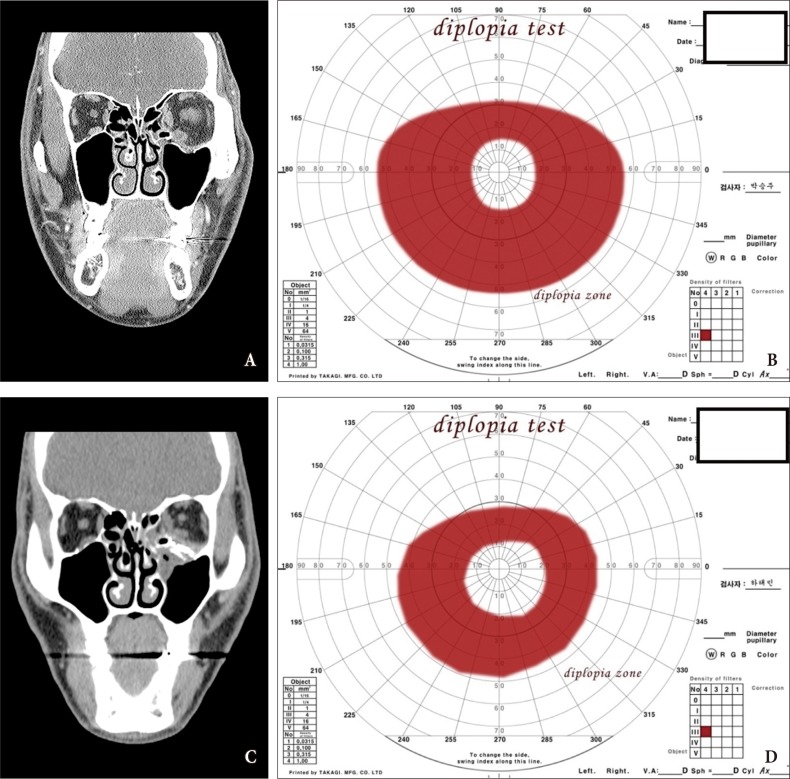
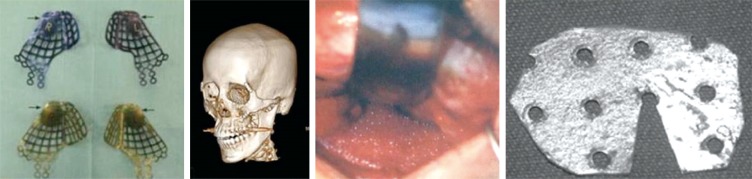
The medial wall and floor of the bony orbit are frequently fractured because of the delicate anatomy. To optimize functional and aesthetic results, reconstructive surgeons should understand the anatomy and pathophysiology of orbital fractures. Appropriate treatment involves optimal timing of intervention, proper indications for operative repair, incision and dissection, release of herniated tissue, implant material and placement, and wound closure. The following review will discuss the management of orbital floor fractures, with the operative method preferred by the author. Special considerations in operation technique and the complication are also present in this article.
Keywords: Blow-out fractures; Complications; Orbital fractures; Surgery.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Nakamura T, Gross CW. Facial fractures: analysis of five years of experience. Arch Otolaryngol. 1973;97:288–290. - PubMed
-
- Gwyn PP, Carraway JH, Horton CE, Adamson JE, Mladick RA. Facial fractures: associated injuries and complications. Plast Reconstr Surg. 1971;47:225–230. - PubMed
-
- Rontal E, Rontal M, Guilford FT. Surgical anatomy of the orbit. Ann Otol Rhinol Laryngol. 1979;88:382–386. - PubMed
-
- Rootman J. Basic anatomic considerations. In: Rootman J, editor. Diseases of the orbit : a multidisciplinary approach. Philadelphia: Lippincott; 1988. pp. 3–18.
-
- Ellis E, 3rd, el-Attar A, Moos KF. An analysis of 2,067 cases of zygomatico-orbital fracture. J Oral Maxillofac Surg. 1985;43:417–428. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
