

DEVOTE 3: temporal relationships between severe hypoglycaemia, cardiovascular outcomes and mortality
- PMID: 28913543
- PMCID: PMC6002964
- DOI: 10.1007/s00125-017-4422-0
DEVOTE 3: temporal relationships between severe hypoglycaemia, cardiovascular outcomes and mortality
Abstract
Aims/hypothesis: The double-blind Trial Comparing Cardiovascular Safety of Insulin Degludec vs Insulin Glargine in Patients with Type 2 Diabetes at High Risk of Cardiovascular Events (DEVOTE) assessed the cardiovascular safety of insulin degludec. The incidence and rates of adjudicated severe hypoglycaemia, and all-cause mortality were also determined. This paper reports a secondary analysis investigating associations of severe hypoglycaemia with cardiovascular outcomes and mortality.
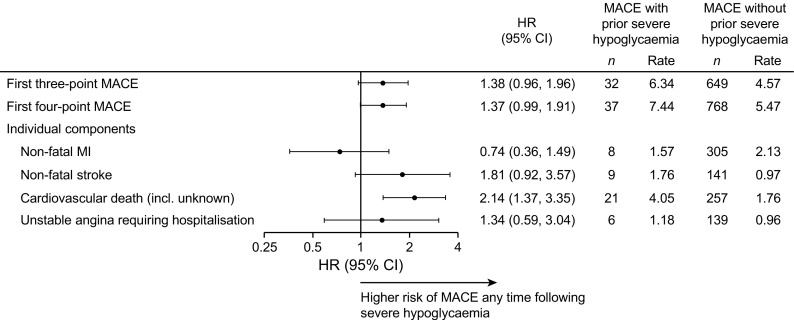
Methods: In DEVOTE, patients with type 2 diabetes were randomised to receive either insulin degludec or insulin glargine U100 (100 units/ml) once daily (between dinner and bedtime) in an event-driven, double-blind, treat-to-target cardiovascular outcomes trial. The primary outcome was the first occurrence of an adjudicated major adverse cardiovascular event (MACE; cardiovascular death, non-fatal myocardial infarction or non-fatal stroke). Adjudicated severe hypoglycaemia was the pre-specified secondary outcome. In the present analysis, the associations of severe hypoglycaemia with both MACE and all-cause mortality was evaluated in the pooled trial population using time-to-event analyses, with severe hypoglycaemia as a time-dependent variable and randomised treatment as a fixed factor. An investigation with interaction terms indicated that the effect of severe hypoglycaemia on the risk of MACE and all-cause mortality were the same for both treatment arms, and so the temporal association for severe hypoglycaemia with subsequent MACE and all-cause mortality is reported for the pooled population.
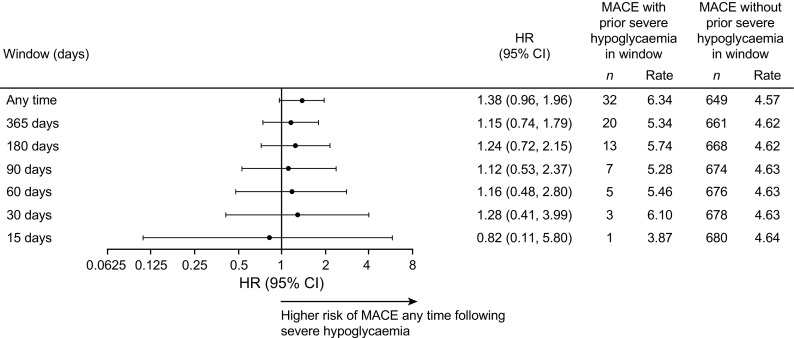
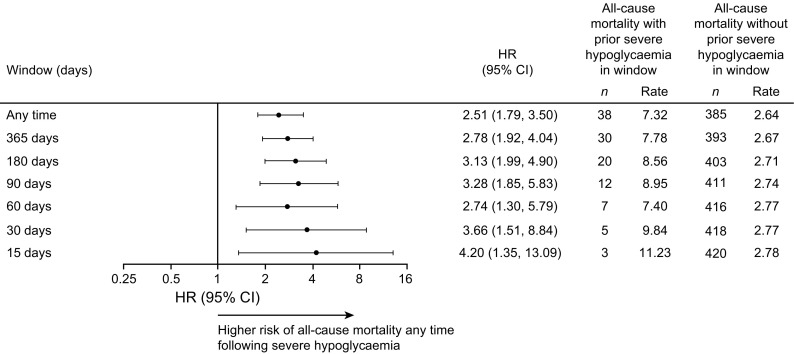
Results: There was a non-significant difference in the risk of MACE for individuals who had vs those who had not experienced severe hypoglycaemia during the trial (HR 1.38, 95% CI 0.96, 1.96; p = 0.080) and therefore there was no temporal relationship between severe hypoglycaemia and MACE. There was a significantly higher risk of all-cause mortality for patients who had vs those who had not experienced severe hypoglycaemia during the trial (HR 2.51, 95% CI 1.79, 3.50; p < 0.001). There was a higher risk of all-cause mortality 15, 30, 60, 90, 180 and 365 days after experiencing severe hypoglycaemia compared with not experiencing severe hypoglycaemia in the same time interval. The association between severe hypoglycaemia and all-cause mortality was maintained after adjustment for the following baseline characteristics: age, sex, HbA1c, BMI, diabetes duration, insulin regimen, hepatic impairment, renal status and cardiovascular risk group.
Conclusions/interpretation: The results from these analyses demonstrate an association between severe hypoglycaemia and all-cause mortality. Furthermore, they indicate that patients who experienced severe hypoglycaemia were particularly at greater risk of death in the short term after the hypoglycaemic episode. These findings indicate that severe hypoglycaemia is associated with higher subsequent mortality; however, they cannot answer the question as to whether severe hypoglycaemia serves as a risk marker for adverse outcomes or whether there is a direct causal effect.
Trial registration: ClinicalTrials.gov NCT01959529.
Keywords: Hypoglycaemia; Insulin therapy; Macrovascular disease.
Conflict of interest statement
Data availability
The data generated during and/or analysed during the current trial are available from the corresponding author on reasonable request.
Funding
This trial and secondary analysis was sponsored and funded by Novo Nordisk (Bagsvaerd, Denmark). JBB received support from The National Institutes of Health (UL1TR001111). The trial sponsor was involved in the design of the trial; the collection, and analysis of data; and writing the clinical report.
Duality of interest
TRP has received research support from Novo Nordisk and AstraZeneca (paid directly to the Medical University of Graz); personal fees as a consultant from AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Novo Nordisk and Roche Diabetes Care. TRP is also the Chief Scientific Officer of CBmed (Center for Biomarker Research in Medicine), a public-funded biomarker research company.
SPM has received personal fees from Abbott Vascular, Novo Nordisk, University of Oxford, AstraZeneca and Bristol-Myers Squibb; and research support from Novo Nordisk, The Medicines Company and Terumo Medical.
DKM has received personal fees from Boehringer Ingelheim, Janssen Research and Development LLC, Sanofi US, Merck Sharp and Dohme Corp., Eli Lilly USA, Novo Nordisk, GlaxoSmithKline, AstraZeneca, Lexicon Pharmaceuticals, Eisai and Esperion.
BZ has received grant support from Boehringer Ingelheim, AstraZeneca and Novo Nordisk; and consulting fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck, Novo Nordisk and Sanofi.
NRP has received personal fees from Servier, Takeda, Novo Nordisk and AstraZeneca in relation to speakers’ fees and advisory board activities (concerning diabetes mellitus); and research grants for his research group (relating to type 2 diabetes mellitus) from Diabetes UK, National Institute for Health Research Efficacy and Mechanism Evaluation (NIHR EME), Julius Clinical and the British Heart Foundation.
SSE has received personal fees related to Data Monitoring Committees from CTI BioPharma, Arena Pharmaceuticals, SFJ Pharmaceuticals, BioMarin, Medivation, Biom’up, Dynavax, Genentech, GlaxoSmithKline, Janssen Research, Novartis, Novo Nordisk, Pfizer, Roche, Sarepta Therapeutics and Xoma; personal fees related to other statistical consulting from AstraZeneca, Celltrion, Sprout Pharmaceuticals, Sanofi, Collegium Pharmaceutical, Intercept, Coherus BioMedical and Emmaus Life Sciences; and research grant support from National Heart, Lung, and Blood Institute (NHLBI).
REP’s services were paid directly to Florida Hospital, a non-profit organisation. Consultancy and speaker fees from AstraZeneca, Takeda and Novo Nordisk; consultancy fees from Boehringer Ingelheim, GlaxoSmithKline, Hanmi Pharmaceutical Co. Ltd., Janssen Scientific Affairs LLC, Ligand Pharmaceuticals, Inc., Eli Lilly, Merck, Pfizer, Eisai, Inc.; research grant from Gilead Sciences, Lexicon Pharmaceuticals, Ligand Pharmaceuticals, Inc., Eli Lilly, Merck, Sanofi US LLC and Takeda.
VW has received personal fees in relation to speakers’ fees and advisory board activities from Novo Nordisk, Eli Lilly, Sanofi, AstraZeneca, Boehringer Ingelheim and Merck; he also reports serving as an investigator for clinical trials sponsored by Merck, Novo Nordisk, Eli Lilly, Sanofi, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Locemia Solutions.
SH has served on speaker panels for Sanofi, Eli Lilly, Takeda, Novo Nordisk and AstraZeneca, for which he has received remuneration. He has served on advisory panels or as a consultant for Boehringer Ingelheim, Novo Nordisk, Eli Lilly and Takeda for which his institution has received remuneration.
ML, KBF, AM, JBL, LL and KK are full-time employees of, and hold stock in, Novo Nordisk A/S.
JBB reports receiving contracted consulting fees, paid to his institution, and travel support from Novo Nordisk, Eli Lilly, GI Dynamics, Elcylex, Merck, Metavention, vTv Pharma, PhaseBio, AstraZeneca, Dance Biopharm, Sanofi, Lexicon Pharmaceuticals, Orexigen, Takeda, Adocia, Roche, NovaTarg, Shenzen HighTide, Fractyl and Dexcom; grant support from Eli Lilly, Bristol-Myers Squibb, GI Dynamics, Merck, PhaseBio, AstraZeneca, Medtronic Minimed, Sanofi, Johnson & Johnson, Andromeda, Boehringer Ingelheim, GlaxoSmithKline, MacroGenics, Intarcia Therapeutics, Lexicon Pharmaceuticals, Scion NeuroStim, Orexigen, Takeda, Theracos and Bayer; he also reports receiving fees and holding stock options in PhaseBio and Insulin Algorithms; he also reports serving on the board of the AstraZeneca Healthcare Foundation.
Contribution statement
All authors confirm that they meet the International Committee of Medical Journal Editors uniform requirements for authorship. Specifically, all authors made substantial contributions to the interpretation of data for the manuscript, drafted and critically revised the manuscript, provided final approval of the version to be published and agreed to be accountable for all aspects of the manuscript. All authors had access to the final results and vouch for the fidelity of the trial to the protocol. Medical writing and editorial support, under the guidance of the authors, was provided by Watermeadow Medical, an Ashfield company, part of UDG Healthcare plc, funded by Novo Nordisk. All authors are responsible for the integrity of the work as a whole.
Figures
References
-
- Dailey G. Overall mortality in diabetes mellitus: where do we stand today? Diabetes Technol Ther. 2011;13(Suppl. 1):S65–S74. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
