

Microsurgical versus endoscopic transsphenoidal resection for acromegaly: a systematic review of outcomes and complications
- PMID: 28913667
- PMCID: PMC6558977
- DOI: 10.1007/s00701-017-3318-6
Microsurgical versus endoscopic transsphenoidal resection for acromegaly: a systematic review of outcomes and complications
Abstract
Purpose: The aim of this systematic review is to evaluate the long-term endocrine outcomes and postoperative complications following endoscopic vs. microscopic transsphenoidal resection (TSR) for the treatment of acromegaly.
Methods: A literature review was performed, and studies with at least five patients who underwent TSR for acromegaly, reporting biochemical remission criteria and long-term remission outcomes were included. Data extracted from each study included surgical technique, perioperative complications, biochemical remission criteria, and long-term remission outcomes.
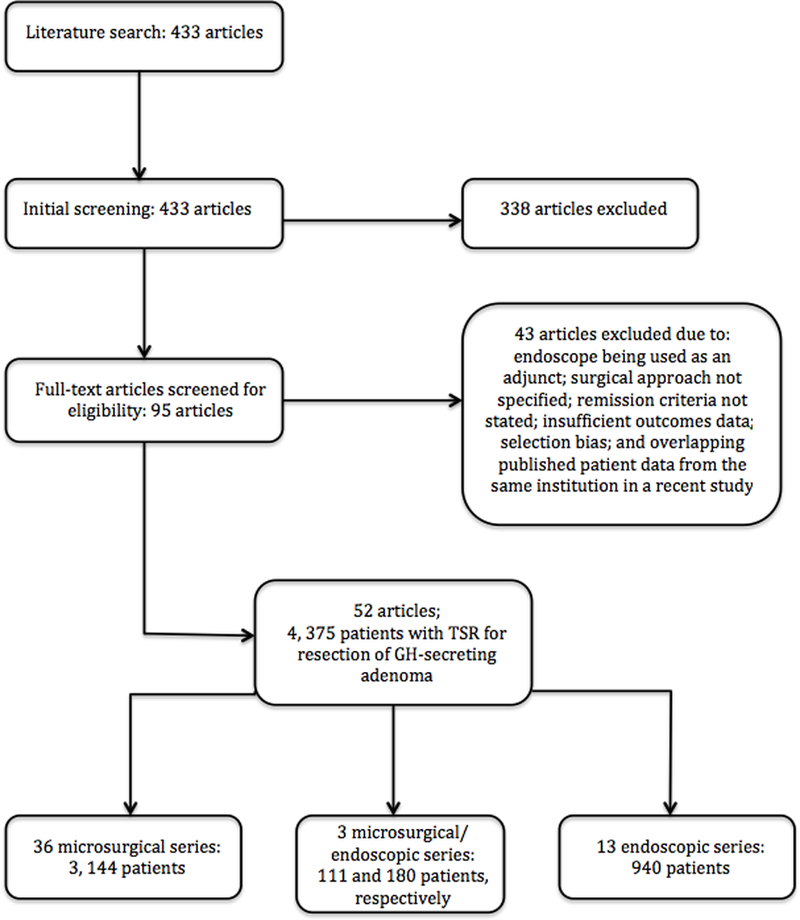
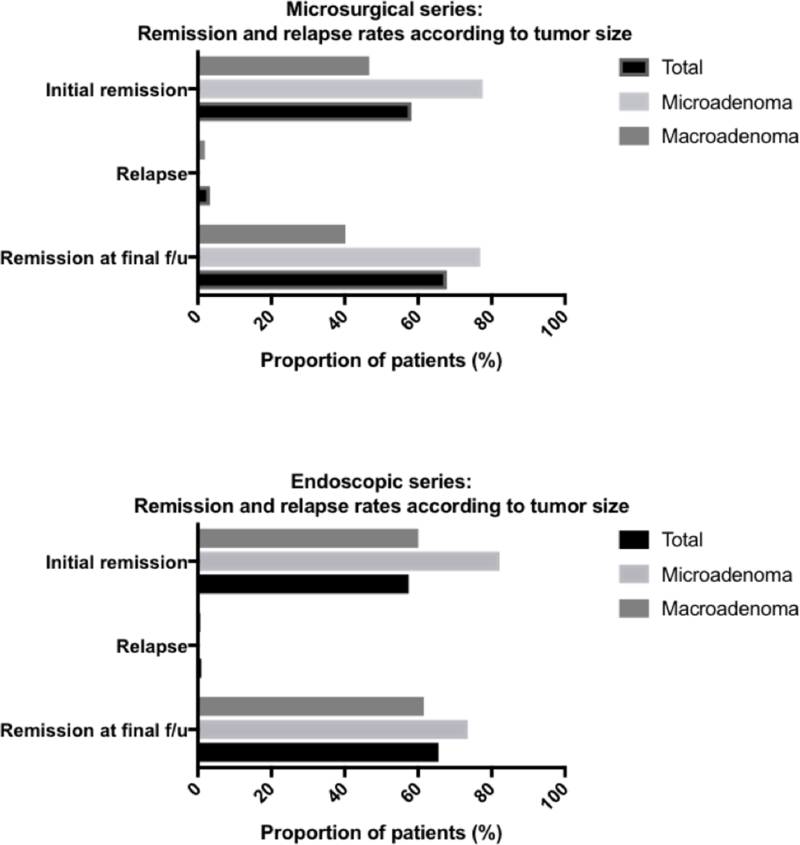
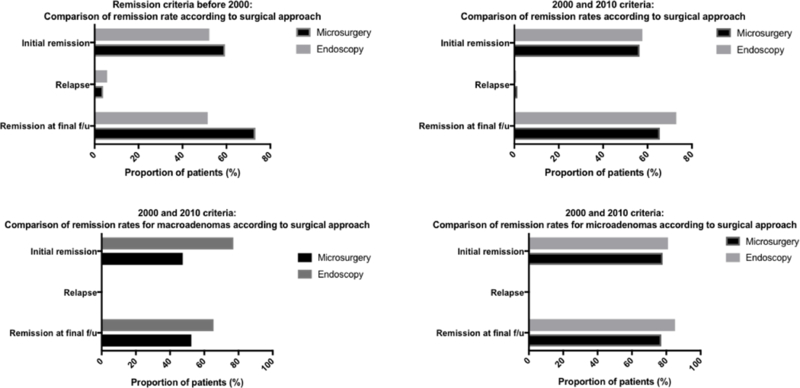
Results: Fifty-two case series from 1976 to 2016 met the inclusion criteria, comprising 4375 patients. Thirty-six reports were microsurgical (n = 3144) and 13 were endoscopic (n = 940). Three studies compared microsurgical (n = 111) to endoscopic TSR outcomes (n = 180). The overall initial and long-term remission rates were 58.2 vs. 57.4% and 69.2 vs. 70.2% for the microsurgical and endoscopic groups, respectively. For microadenomas, the initial and long-term remission rates were 77.6 vs. 82.2% and 76.9 vs. 73.5% for microsurgical and endoscopic approaches, respectively. For macroadenomas, the initial and long-term remission rates were 46.9 vs. 60.0% and 40.2 vs. 61.5% for microsurgical and endoscopic approaches, respectively. The rates of postoperative CSF leak were 3.0 vs. 2.3% for the microscopic and endoscopic groups, respectively. The rates of hypopituitarism and transient diabetes insipidus were 6.7 vs. 6.4% and 9.0 vs. 7.8% for the microscopic and endoscopic groups, respectively.
Conclusions: Both endoscopic and microsurgical approaches for TSR of growth hormone-secreting adenomas are viable treatment options for patients with acromegaly, and yield similarly high rates of remission under the most current consensus criteria.
Keywords: Acromegaly; Endoscopic; Growth hormone; Microscopic; Pituitary adenoma; Review; Transsphenoidal.
Conflict of interest statement
Figures
References
-
- Melmed S, Colao A, Barkan A, Molitch M, Grossman AB, Kleinberg D, Clemmons D, Chanson P, Laws E, Schlechte J, Vance ML, Ho K, Giustina A, Acromegaly Consensus G (2009) Guidelines for acromegaly management: an update. J Clin Endocrinol Metab 94:1509–1517 - PubMed
-
- Katznelson L (2010) Approach to the patient with persistent acromegaly after pituitary surgery. J Clin Endocrinol Metab 95:4114–4123 - PubMed
-
- McLanaham CS, Christy JH, Tindall GT (1978) Anterior pituitary function before and after trans-sphenoidal microsurgical resection of pituitary tumors. Neurosurgery 3:142–145 - PubMed
-
- Ciric I, Ragin A, Baumgartner C, Pierce D (1997) Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 40:225–236; discussion 236–227 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
