

The impact of cardiovascular co-morbidities and duration of diabetes on the association between microvascular function and glycaemic control
- PMID: 28915818
- PMCID: PMC5603035
- DOI: 10.1186/s12933-017-0594-7
The impact of cardiovascular co-morbidities and duration of diabetes on the association between microvascular function and glycaemic control
Abstract
Background: Good glycaemic control in type 2 diabetes (T2DM) protects the microcirculation. Current guidelines suggest glycaemic targets be relaxed in advanced diabetes. We explored whether disease duration or pre-existing macrovascular complications attenuated the association between hyperglycaemia and microvascular function.
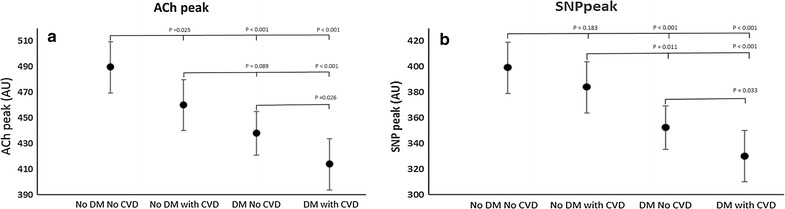
Methods: 743 participants with T2DM (n = 222), cardiovascular disease (CVD = 183), both (n = 177) or neither (controls = 161) from two centres in the UK, underwent standard clinical measures and endothelial dependent (ACh) and independent (SNP) microvascular function assessment using laser Doppler imaging.
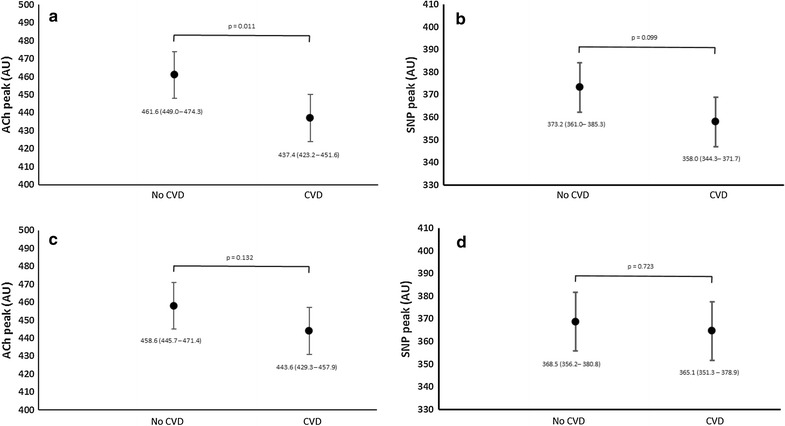
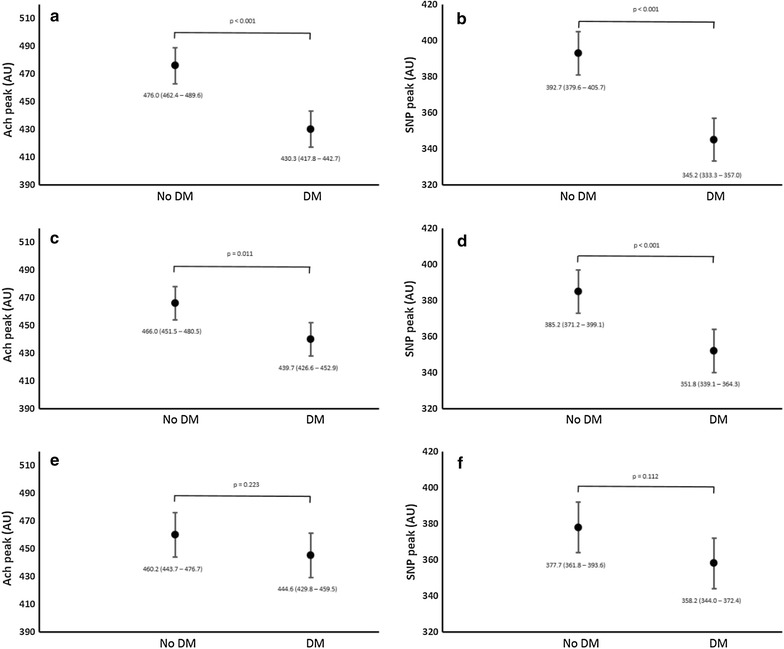
Results: People with T2DM and CVD had attenuated ACh and SNP responses compared to controls. This was additive in those with both (ANOVA p < 0.001). In regression models, cardiovascular risk factors accounted for attenuated ACh and SNP responses in CVD, whereas HbA1c accounted for the effects of T2DM. HbA1c was associated with ACh and SNP response after adjustment for cardiovascular risk factors (adjusted standardised beta (β) -0.096, p = <0.008 and -0.135, p < 0.001, respectively). Pre-existing CVD did not modify this association (β -0.099; p = 0.006 and -0.138; p < 0.001, respectively). Duration of diabetes accounted for the association between HbA1c and ACh (β -0.043; p = 0.3), but not between HbA1c and SNP (β -0.105; p = 0.02).
Conclusions: In those with T2DM and CVD, good glycaemic control is still associated with better microvascular function, whereas in those with prolonged disease this association is lost. This suggests duration of diabetes may be a better surrogate for "advanced disease" than concomitant CVD, although this requires prospective validation.
Keywords: Cardiovascular disease; Diabetes; Glycaemic legacy; Microcirculation.
Figures
References
-
- Group UPDSU Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK prospective diabetes study (UKPDS) group. Lancet. 1998;352(9131):837–853. doi: 10.1016/S0140-6736(98)07019-6. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
