

Physician-staffed helicopter emergency medical service has a beneficial impact on the incidence of prehospital hypoxia and secured airways on patients with severe traumatic brain injury
- PMID: 28915898
- PMCID: PMC5603088
- DOI: 10.1186/s13049-017-0438-1
Physician-staffed helicopter emergency medical service has a beneficial impact on the incidence of prehospital hypoxia and secured airways on patients with severe traumatic brain injury
Abstract
Background: After traumatic brain injury (TBI), hypotension, hypoxia and hypercapnia have been shown to result in secondary brain injury that can lead to increased mortality and disability. Effective prehospital assessment and treatment by emergency medical service (EMS) is considered essential for favourable outcome. The aim of this study was to evaluate the effect of a physician-staffed helicopter emergency medical service (HEMS) in the treatment of TBI patients.
Methods: This was a retrospective cohort study. Prehospital data from two periods were collected: before (EMS group) and after (HEMS group) the implementation of a physician-staffed HEMS. Unconscious prehospital patients due to severe TBI were included in the study. Unconsciousness was defined as a Glasgow coma scale (GCS) score ≤ 8 and was documented either on-scene, during transportation or by an on-call neurosurgeon on hospital admission. Modified Glasgow Outcome Score (GOS) was used for assessment of six-month neurological outcome and good neurological outcome was defined as GOS 4-5.
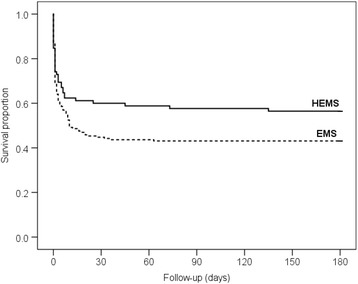
Results: Data from 181 patients in the EMS group and 85 patients in the HEMS group were available for neurological outcome analyses. The baseline characteristics and the first recorded vital signs of the two cohorts were similar. Good neurological outcome was more frequent in the HEMS group; 42% of the HEMS managed patients and 28% (p = 0.022) of the EMS managed patients had a good neurological recovery. The airway was more frequently secured in the HEMS group (p < 0.001). On arrival at the emergency department, the patients in the HEMS group were less often hypoxic (p = 0.024). In univariate analysis HEMS period, lower age and secured airway were associated with good neurological outcome.
Conclusion: The introduction of a physician-staffed HEMS unit resulted in decreased incidence of prehospital hypoxia and increased the number of secured airways. This may have contributed to the observed improved neurological outcome during the HEMS period.
Trial registration: ClinicalTrials.gov IDNCT02659046. Registered January 15th, 2016.
Keywords: Airway management (MeSH); Critical care (MeSH); Emergency medical services (MeSH); Endotracheal intubation (MeSH); Glasgow outcome scale (MeSH); Patient outcome assessment (MeSH); Prehospital emergency care (MeSH); Traumatic brain injury (MeSH).
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Regional Ethics Committee of the Pirkanmaa Hospital District (reference number R15158), permission to conduct the study was obtained from the Research Director of Tampere University Hospital and registered in
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Pre-hospital severe traumatic brain injury - comparison of outcome in paramedic versus physician staffed emergency medical services.Scand J Trauma Resusc Emerg Med. 2016 Apr 29;24:62. doi: 10.1186/s13049-016-0256-x. Scand J Trauma Resusc Emerg Med. 2016. PMID: 27130216 Free PMC article. Clinical Trial.
-
Prehospital on-scene anaesthetist treating severe traumatic brain injury patients is associated with lower mortality and better neurological outcome.Scand J Trauma Resusc Emerg Med. 2019 Jan 28;27(1):9. doi: 10.1186/s13049-019-0590-x. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30691530 Free PMC article.
-
Effects of physician-based emergency medical service dispatch in severe traumatic brain injury on prehospital run time.Injury. 2012 Nov;43(11):1838-42. doi: 10.1016/j.injury.2012.05.020. Epub 2012 Jun 12. Injury. 2012. PMID: 22695322
-
Effect of Physician-Staffed Emergency Medical Services (P-EMS) on the Outcome of Patients with Severe Traumatic Brain Injury: A Review of the Literature.Prehosp Emerg Care. 2019 Sep-Oct;23(5):730-739. doi: 10.1080/10903127.2019.1575498. Epub 2019 Mar 15. Prehosp Emerg Care. 2019. PMID: 30693835 Review.
-
The cost-effectiveness of physician staffed Helicopter Emergency Medical Service (HEMS) transport to a major trauma centre in NSW, Australia.Injury. 2012 Nov;43(11):1843-9. doi: 10.1016/j.injury.2012.07.184. Epub 2012 Aug 13. Injury. 2012. PMID: 22898559 Review.
Cited by
-
Pre-hospital endotracheal intubation in severe traumatic brain injury: ventilation targets and mortality-a retrospective analysis of 308 patients.Scand J Trauma Resusc Emerg Med. 2023 Sep 12;31(1):46. doi: 10.1186/s13049-023-01115-8. Scand J Trauma Resusc Emerg Med. 2023. PMID: 37700380 Free PMC article.
-
Treatment of pediatric patients with traumatic brain injury by Dutch Helicopter Emergency Medical Services (HEMS).PLoS One. 2022 Dec 30;17(12):e0277528. doi: 10.1371/journal.pone.0277528. eCollection 2022. PLoS One. 2022. PMID: 36584019 Free PMC article.
-
Prehospital triage for mass casualty incidents using the META method for early surgical assessment: retrospective validation of a hospital trauma registry.Eur J Trauma Emerg Surg. 2020 Apr;46(2):425-433. doi: 10.1007/s00068-018-1040-6. Epub 2018 Nov 7. Eur J Trauma Emerg Surg. 2020. PMID: 30406394
-
Association of Pre-Hospital Helicopter Transport with Reduced Mortality in Traumatic Brain Injury in Japan: A Nationwide Retrospective Cohort Study.J Neurotrauma. 2022 Jan;39(1-2):76-85. doi: 10.1089/neu.2021.0181. Epub 2021 Dec 1. J Neurotrauma. 2022. PMID: 34779275 Free PMC article.
-
Causes of death and characteristics of non-survivors rescued during recreational mountain activities in Japan between 2011 and 2015: a retrospective analysis.BMJ Open. 2022 Feb 3;12(2):e053935. doi: 10.1136/bmjopen-2021-053935. BMJ Open. 2022. PMID: 35115353 Free PMC article.
References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
