

Neurological outcomes and duration from cardiac arrest to the initiation of extracorporeal membrane oxygenation in patients with out-of-hospital cardiac arrest: a retrospective study
- PMID: 28915913
- PMCID: PMC5603067
- DOI: 10.1186/s13049-017-0440-7
Neurological outcomes and duration from cardiac arrest to the initiation of extracorporeal membrane oxygenation in patients with out-of-hospital cardiac arrest: a retrospective study
Abstract
Background: We investigated the relationship between neurological outcomes and duration from cardiac arrest (CA) to the initiation of extracorporeal membrane oxygenation (ECMO) (CA-to-ECMO) in patients with out-of-hospital cardiac arrest (OHCA) treated with extracorporeal cardiopulmonary resuscitation (ECPR) and determined the ideal time at which ECPR should be performed.
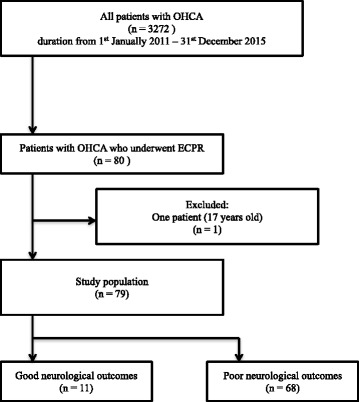
Methods: During the time period in which this study was conducted, 3451 patients experienced OHCA. This study finally included 79 patients aged 18 years or older whose OHCA had been witnessed and who underwent ECPR in the emergency room between January 2011 and December 2015. Our primary endpoint was survival to hospital discharge with good neurological outcomes (a cerebral performance category of 1 or 2).
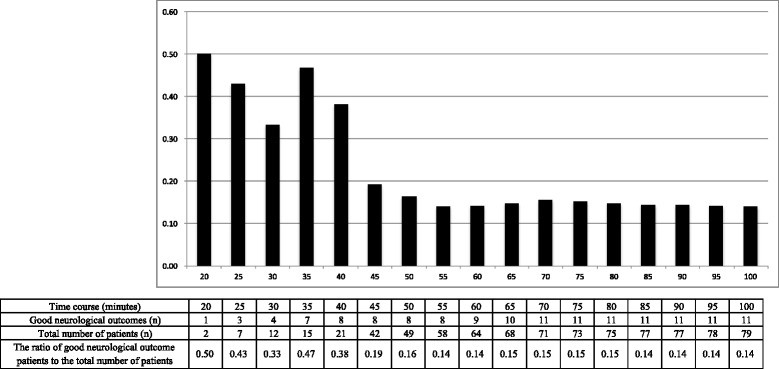
Results: Of the 79 patients included, 11 had good neurological outcomes. The median duration from CA-to-ECMO was significantly shorter in the good neurological outcome group (33 min, interquartile range [IQR], 27-50 vs. 46 min, IQR, 42-56: p = 0.03). After controlling for potential confounders, we found that the adjusted odds ratio of CA-to-ECMO time for a good neurological outcome was 0.92 (95% confidence interval: 0.87-0.98, p = 0.007). The area under the receiver operating characteristic curve of CA-to-ECMO for predicting a good neurological outcome was 0.71, and the optimal CA-to-ECMO cutoff time was 40 min. The dynamic probability of survival with good neurological outcomes based on CA-to-ECMO time showed that the survival rate with good neurological outcome decreased abruptly from over 30% to approximately 15% when the CA-to-ECMO time exceeded 40 min.
Discussion: In this study, CA-to-ECMO time was significantly shorter among patients with good neurological outcomes, and significantly associated with good neurological outcomes at hospital discharge. In addition, the probability of survival with good neurological outcome decreased when the CA-to-ECMO time exceeded 40 minutes. The indication for ECPR for patients with OHCA should include several factors. However, the duration of CPR before the initiation of ECMO is a key factor and an independent factor for good neurological outcomes in patients with OHCA treated with ECPR. Therefore, the upper limit of CA-to-ECMO time should be inevitably included in the indication for ECPR for patients with OHCA. In the present study, there was a large difference in the rate of survival to hospital discharge with good neurological outcome between the patients with a CA-to-ECMO time within 40 minutes and those whose time was over 40 minutes. Based on the present study, the time limit of the duration of CPR before the initiation of ECMO might be around 40 minutes. We should consider ECPR in patients with OHCA if they are relatively young, have a witness and no terminal disease, and the initiation of ECMO is presumed to be within this time period.
Conclusions: The duration from CA-to-ECMO was significantly associated with good neurological outcomes. The indication for patients with OHCA should include a criterion for the ideal time to initiate ECPR.
Keywords: Cardiac arrest; Extracorporeal cardiopulmonary resuscitation; Extracorporeal membrane oxygenation; Neurological outcome.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the institutional review board of Tokyo Metropolitan Bokutoh Hospital, with a waiver of informed consent to protect participant anonymity. The ethics committee’s reference number for the study was 61.
Consent for publication
Not applicable. No individual patient data has been reported.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Chen YS, Lin JW, Yu HY, Ko WJ, Jerng JS, Chang WT, et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008;372:554–561. doi: 10.1016/S0140-6736(08)60958-7. - DOI - PubMed
-
- Sakamoto T, Morimura N, Nagao K, Asai Y, Yokota H, Nara S, et al. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: a prospective observational study. Resuscitation. 2014;85:762–768. doi: 10.1016/j.resuscitation.2014.01.031. - DOI - PubMed
-
- Tonna JE, Johnson NJ, Greenwood J, Gaieski DF, Shinar Z, Bellezo JM, et al. Practice characteristics of emergency department extracorporeal cardiopulmonary resuscitation (eCPR) programs in the United States: the current state of the art of emergency department extracorporeal membrane oxygenation (ED ECMO) Resuscitation. 2016;107:38–46. doi: 10.1016/j.resuscitation.2016.07.237. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
