

Sex differences in the prevalence of genetic mutations in FTD and ALS: A meta-analysis
- PMID: 28916533
- PMCID: PMC5634668
- DOI: 10.1212/WNL.0000000000004494
Sex differences in the prevalence of genetic mutations in FTD and ALS: A meta-analysis
Abstract
Objective: To conduct a meta-analysis that investigates sex differences in the prevalence of mutations in the 3 most common genes that cause amyotrophic lateral sclerosis (ALS) and frontotemporal dementia (FTD)-chromosome 9 open reading frame 72 (C9orf72), progranulin (GRN), or microtubule-associated protein tau (MAPT)-in patients clinically diagnosed with these conditions.
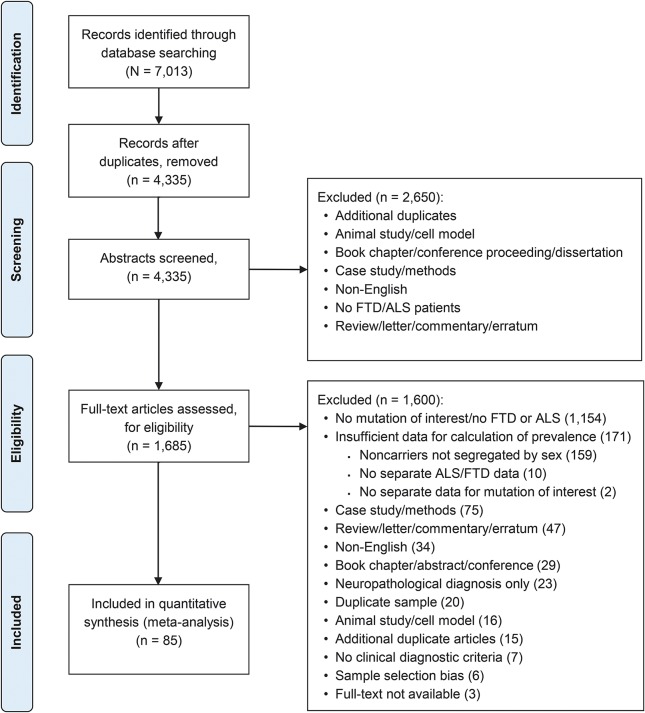
Methods: MEDLINE, EMBASE, and PsycINFO databases were searched (inception to June 30, 2016). Studies of patients with FTD or ALS that reported the number of men and women with and without mutations of interest were selected. Female to male pooled risk ratios (RR) and 95% confidence intervals (CI) for each mutation were calculated using random-effects models.
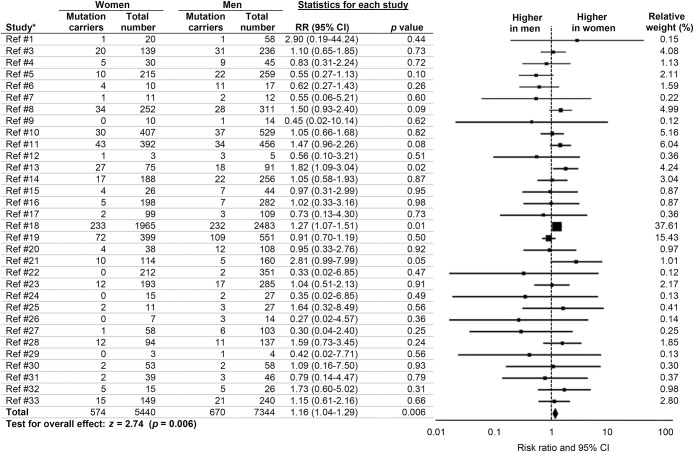
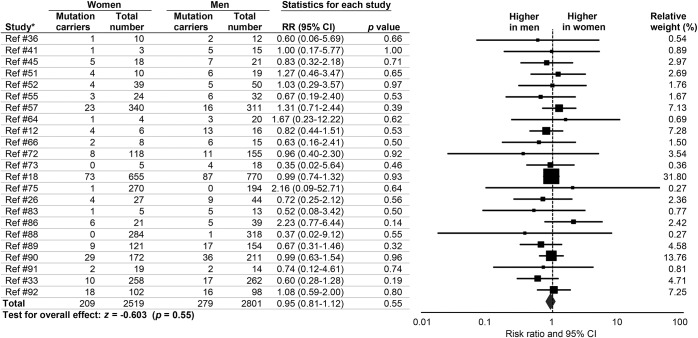
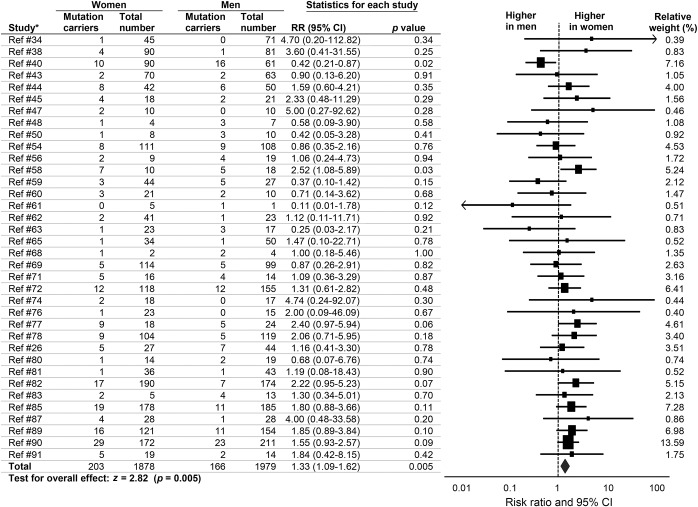
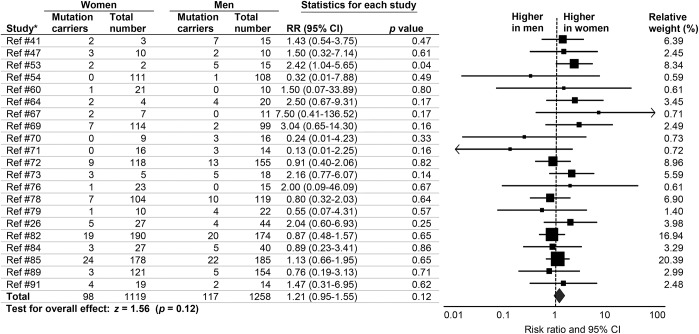
Results: Thirty-two articles reporting 12,784 patients with ALS (including 1,244 C9orf72 mutation carriers) revealed a higher prevalence of female patients with C9orf72-related ALS (RR 1.16, 95% CI 1.04-1.29). Twenty-three articles reporting 5,320 patients with FTD (including 488 C9orf72 mutation carriers) revealed no sex differences in C9orf72-related FTD (RR 0.95, 95% CI 0.81-1.12). Thirty-six articles reporting 3,857 patients with FTD (including 369 GRN mutation carriers) revealed a higher prevalence of female patients with GRN-related FTD (RR 1.33, 95% CI 1.09-1.62). Finally, 21 articles reporting 2,377 patients with FTD (including 215 MAPT mutation carriers) revealed no sex difference in MAPT-related FTD (RR 1.21, 95% CI 0.95-1.55).
Conclusions: Higher female prevalence of C9orf72 hexanucleotide repeat expansions in ALS and GRN mutations in FTD suggest that sex-related risk factors might moderate C9orf72 and GRN-mediated phenotypic expression.
© 2017 American Academy of Neurology.
Figures
References
-
- McKhann GM, Albert MS, Grossman M, Miller B, Dickson D, Trojanowski JQ. Clinical and pathological diagnosis of frontotemporal dementia: report of the work group on frontotemporal dementia and Pick's disease. Arch Neurol 2001;58:1803–1809. - PubMed
-
- Mehta P, Kaye W, Bryan L, et al. . Prevalence of amyotrophic lateral sclerosis: United States, 2012–2013. MMWR Surveill Summ 2016;65:1–12. - PubMed
-
- Itzcovich T, Xi Z, Martinetto H, et al. . Analysis of C9orf72 in patients with frontotemporal dementia and amyotrophic lateral sclerosis from Argentina. Neurobiol Aging 2016;40:192.e113–192.e115. - PubMed
-
- Bruijn LI, Miller TM, Cleveland DW. Unraveling the mechanisms involved in motor neuron degeneration in ALS. Annu Rev Neurosci 2004;27:723–749. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous