

Risk Stratification Model: Lower-Extremity Ultrasonography for Hospitalized Patients with Suspected Deep Vein Thrombosis
- PMID: 28916935
- PMCID: PMC5756163
- DOI: 10.1007/s11606-017-4170-3
Risk Stratification Model: Lower-Extremity Ultrasonography for Hospitalized Patients with Suspected Deep Vein Thrombosis
Abstract
Background: The Wells score for deep venous thrombosis (DVT) has a high failure rate and low efficiency among inpatients.
Objective: To create and validate an inpatient-specific risk stratification model to help assess pre-test probability of DVT in hospitalized patients.
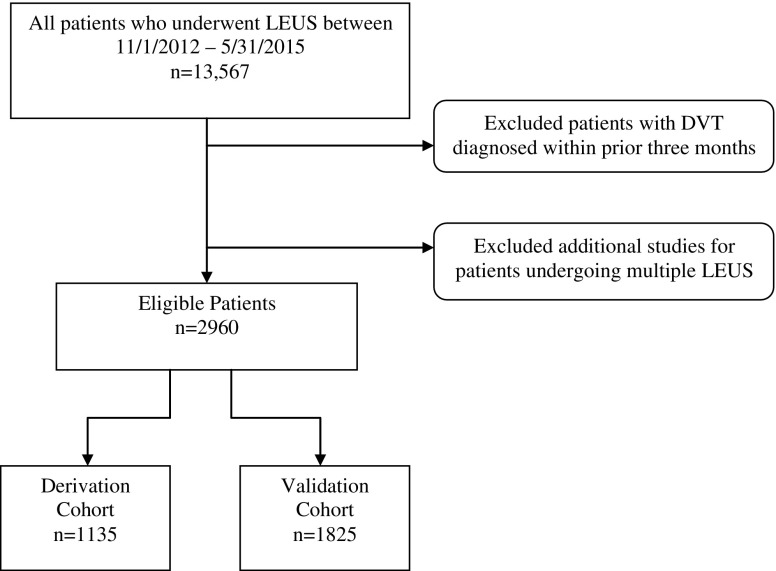
Design: Prospective cohort study of hospitalized patients undergoing lower-extremity ultrasonography studies (LEUS) for suspected DVT. Demographics, physical findings, medical history, medications, hospitalization, and laboratory and imaging results were collected. Samples were divided into model derivation (patients undergoing LEUS 11/1/2012-12/31/2013) and validation cohorts (LEUS 1/1/2014-5/31/2015). A DVT prediction rule was derived using the recursive partitioning algorithm (decision tree-type approach) and was then validated.
Participants: Adult inpatients undergoing LEUS for suspected DVT from November 2012 to May 2015, excluding those with DVT in the prior 3 months, at a 793-bed, urban academic quaternary-care hospital with ~50,000 admissions annually.
Main measures: The primary outcome was the presence of proximal DVT, and the secondary outcome was the presence of any DVT (proximal or distal). Model sensitivity and specificity for predicting DVT were calculated.
Key results: Recursive partitioning yielded four variables (previous DVT, active cancer, hospitalization ≥ 6 days, age ≥ 46 years) that optimized the prediction of proximal DVT and yield in the derivation cohort. From this decision tree, we stratified a scoring system using the validation cohort, categorizing patients into low- and high-risk groups. The incidence rates of proximal DVT were 2.9% and 12.0%, and of any DVT were 5.2% and 21.0%, for the low- and high-risk groups, respectively. The AUC for the discriminatory accuracy of the Center for Evidence-Based Imaging (CEBI) score for risk of proximal DVT identified on LEUS was 0.73. Model sensitivity was 98.1% for proximal and 98.1% for any DVT.
Conclusions: In hospitalized adults, specific factors can help clinicians predict risk of DVT, identifying those with low pre-test probability, in whom ultrasonography can be safely avoided.
Keywords: Wells score; deep vein thrombosis; inpatient; pre-test probability.
Conflict of interest statement
Dr. Piazza has received research grants from Bristol Myers Squibb, Daiichi Sankyo, the Thrombosis Research Institute, and Janssen, and consulting fees from Merck, eXIthera, and Zafgen. Dr. Khorasani is a consultant to Medicalis Corporation. U.S. Patent 6,029,138 is held by Brigham and Women’s Hospital on clinical decision support-related software, licensed to Medicalis Corporation in 2000. As a result of licensing, Brigham and Women’s Hospital and its parent organization, Partners HealthCare, Inc., have equity and royalty interests in Medicalis. The authors have no other relationships or activities that could appear to have influenced the submitted work.
The data sets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Figures


Comment in
-
Refining Risk for Deep Vein Thrombosis in Hospitalized Patients.J Gen Intern Med. 2018 Jan;33(1):6. doi: 10.1007/s11606-017-4194-8. J Gen Intern Med. 2018. PMID: 29043536 Free PMC article. No abstract available.
References
-
- Engelberger RP, Aujesky D, Calanca L, Staeger P, Hugli O, Mazzolai L. Comparison of the diagnostic performance of the original and modified Wells score in inpatients and outpatients with suspected deep vein thrombosis. Thromb Res. 2011;127(6):535–9. doi: 10.1016/j.thromres.2011.02.008. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
