

Return to work and lost earnings after acute respiratory distress syndrome: a 5-year prospective, longitudinal study of long-term survivors
- PMID: 28918401
- PMCID: PMC6002952
- DOI: 10.1136/thoraxjnl-2017-210217
Return to work and lost earnings after acute respiratory distress syndrome: a 5-year prospective, longitudinal study of long-term survivors
Abstract
Background: Delayed return to work is common after acute respiratory distress syndrome (ARDS), but has undergone little detailed evaluation. We examined factors associated with the timing of return to work after ARDS, along with lost earnings and shifts in healthcare coverage.
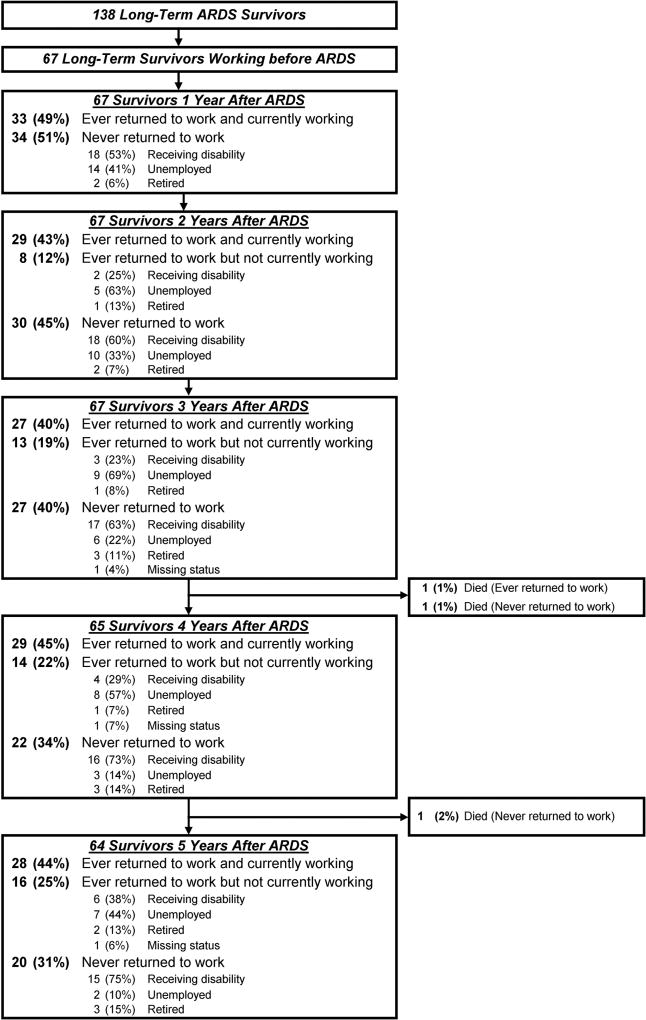
Methods: Five-year, multisite prospective, longitudinal cohort study of 138 2-year ARDS survivors hospitalised between 2004 and 2007. Employment and healthcare coverage were collected via structured interview. Predictors of time to return to work were evaluated using Fine and Grey regression analysis. Lost earnings were estimated using Bureau of Labor Statistics data.
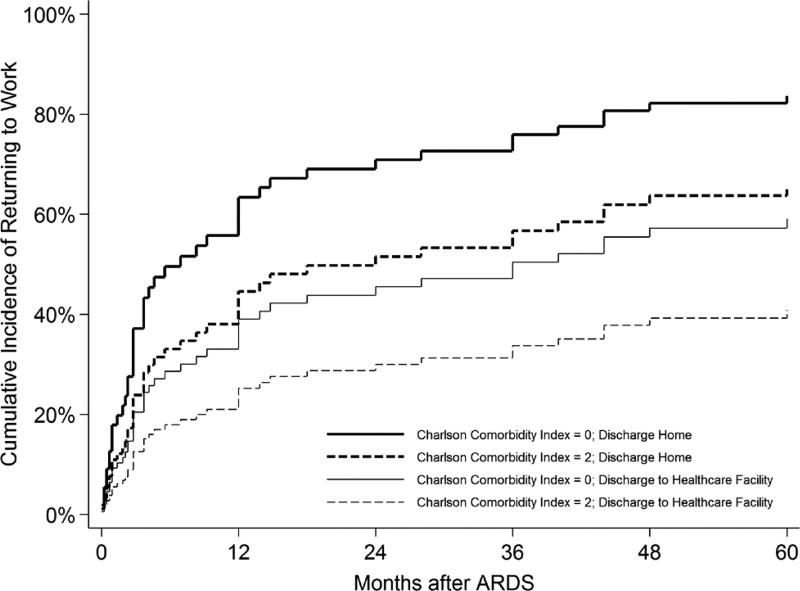
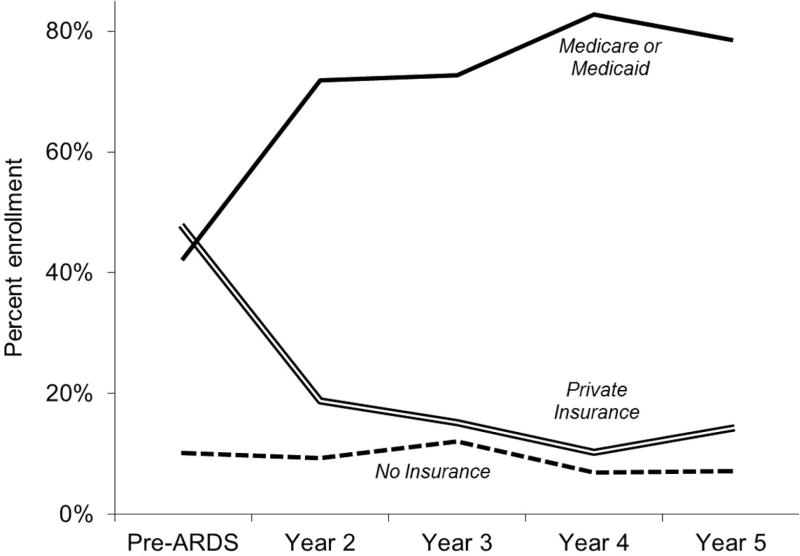
Results: Sixty-seven (49%) of the 138 2-year survivors were employed prior to ARDS. Among 64 5-year survivors, 20 (31%) never returned to work across 5-year follow-up. Predictors of delayed return to work (HR (95% CI)) included baseline Charlson Comorbidity Index (0.77 (0.59 to 0.99) per point; p=0.04), mechanical ventilation duration (0.67 (0.55 to 0.82) per day up to 5 days; p<0.001) and discharge to a healthcare facility (0.49 (0.26 to 0.93); p=0.03). Forty-nine of 64 (77%) 5-year survivors incurred lost earnings, with average (SD) losses ranging from US$38 354 (21,533) to US$43 510 (25,753) per person per year. Jobless, non-retired survivors experienced a 33% decrease in private health insurance and concomitant 37% rise in government-funded coverage.
Conclusions: Across 5-year follow-up, nearly one-third of previously employed ARDS survivors never returned to work. Delayed return to work was associated with patient-related and intensive care unit/hospital-related factors, substantial lost earnings and a marked rise in government-funded healthcare coverage. These important consequences emphasise the need to design and evaluate vocation-based interventions to assist ARDS survivors return to work.
Trial registration: ClinicalTrials.gov NCT00300248.
Keywords: ARDS; acute respiratory distress syndrome; critical illness; employment; health insurance; intensive care unit; return to work; salary.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Joblessness and Lost Earnings after Acute Respiratory Distress Syndrome in a 1-Year National Multicenter Study.Am J Respir Crit Care Med. 2017 Oct 15;196(8):1012-1020. doi: 10.1164/rccm.201611-2327OC. Am J Respir Crit Care Med. 2017. PMID: 28448162 Free PMC article.
-
Physical declines occurring after hospital discharge in ARDS survivors: a 5-year longitudinal study.Intensive Care Med. 2016 Oct;42(10):1557-1566. doi: 10.1007/s00134-016-4530-1. Epub 2016 Sep 16. Intensive Care Med. 2016. PMID: 27637716
-
Influence of quality of intensive care on quality of life/return to work in survivors of the acute respiratory distress syndrome: prospective observational patient cohort study (DACAPO).BMC Public Health. 2020 Jun 5;20(1):861. doi: 10.1186/s12889-020-08943-8. BMC Public Health. 2020. PMID: 32503583 Free PMC article.
-
Return to work after critical illness: a systematic review and meta-analysis.Thorax. 2020 Jan;75(1):17-27. doi: 10.1136/thoraxjnl-2019-213803. Epub 2019 Nov 8. Thorax. 2020. PMID: 31704795 Free PMC article.
-
Long-term outcome after the acute respiratory distress syndrome: different from general critical illness?Curr Opin Crit Care. 2018 Feb;24(1):35-40. doi: 10.1097/MCC.0000000000000476. Curr Opin Crit Care. 2018. PMID: 29189296 Free PMC article. Review.
Cited by
-
Shoulder Impairment Following Critical Illness: A Prospective Cohort Study.Crit Care Med. 2018 Nov;46(11):1769-1774. doi: 10.1097/CCM.0000000000003347. Crit Care Med. 2018. PMID: 30095496 Free PMC article.
-
Disintegration of the NuRD Complex in Primary Human Muscle Stem Cells in Critical Illness Myopathy.Int J Mol Sci. 2023 Feb 1;24(3):2772. doi: 10.3390/ijms24032772. Int J Mol Sci. 2023. PMID: 36769095 Free PMC article.
-
Interrelationships among workload, illness severity, and function on return to work following acute respiratory distress syndrome.Aust Crit Care. 2023 Mar;36(2):247-253. doi: 10.1016/j.aucc.2022.01.002. Epub 2022 Feb 21. Aust Crit Care. 2023. PMID: 35210156 Free PMC article.
-
School and Work Absences After Critical Care Hospitalization for Pediatric Acute Respiratory Failure: A Secondary Analysis of a Cluster Randomized Trial.JAMA Netw Open. 2021 Dec 1;4(12):e2140732. doi: 10.1001/jamanetworkopen.2021.40732. JAMA Netw Open. 2021. PMID: 34940862 Free PMC article. Clinical Trial.
-
Effect of a postoperative home-based exercise and self-management programme on physical function in people with lung cancer (CAPACITY): protocol for a randomised controlled trial.BMJ Open Respir Res. 2022 Jan;9(1):e001189. doi: 10.1136/bmjresp-2021-001189. BMJ Open Respir Res. 2022. PMID: 35039313 Free PMC article.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical