

Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in HIV-infected adults: a prospective cohort study
- PMID: 28919338
- PMCID: PMC5739874
- DOI: 10.1016/S1473-3099(17)30474-7
Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in HIV-infected adults: a prospective cohort study
Abstract
Background: WHO recommends Xpert MTB/RIF as initial diagnostic testing for tuberculous meningitis. However, diagnosis remains difficult, with Xpert sensitivity of about 50-70% and culture sensitivity of about 60%. We evaluated the diagnostic performance of the new Xpert MTB/RIF Ultra (Xpert Ultra) for tuberculous meningitis.
Methods: We prospectively obtained diagnostic cerebrospinal fluid (CSF) specimens during screening for a trial on the treatment of HIV-associated cryptococcal meningitis in Mbarara, Uganda. HIV-infected adults with suspected meningitis (eg, headache, nuchal rigidity, altered mental status) were screened consecutively at Mbarara Regional Referral Hospital. We centrifuged CSF, resuspended the pellet in 2 mL of CSF, and tested 0·5 mL with mycobacteria growth indicator tube culture, 1 mL with Xpert, and cryopreserved 0·5 mL, later tested with Xpert Ultra. We assessed diagnostic performance against uniform clinical case definition or a composite reference standard of any positive CSF tuberculous test.
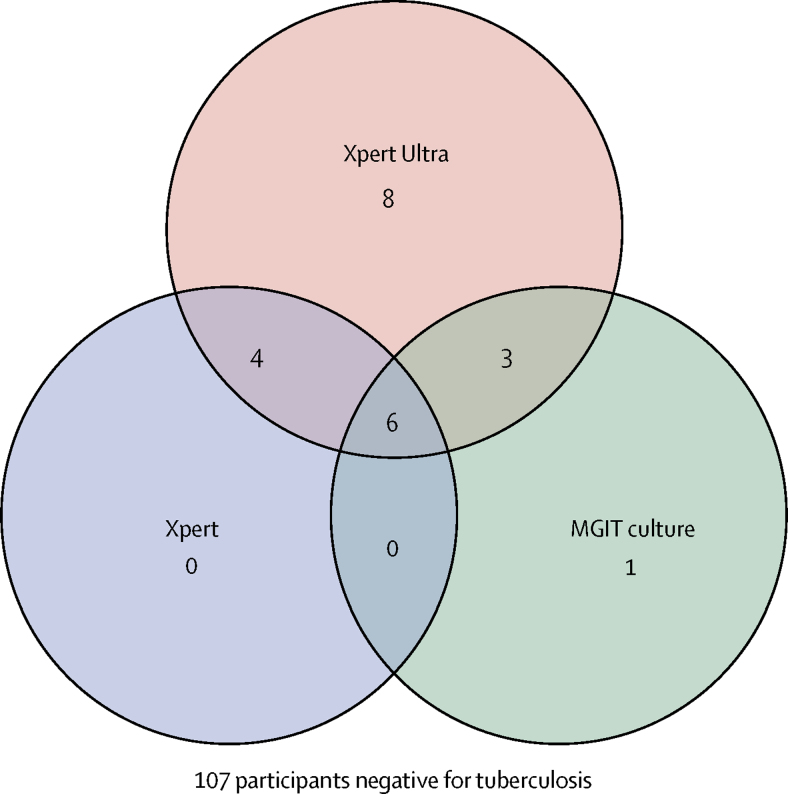
Findings: From Feb 27, 2015, to Nov 7, 2016, we prospectively evaluated 129 HIV-infected adults with suspected meningitis for tuberculosis. 23 participants were classified as probable or definite tuberculous meningitis by uniform case definition, excluding Xpert Ultra results. Xpert Ultra sensitivity was 70% (95% CI 47-87; 16 of 23 cases) for probable or definite tuberculous meningitis compared with 43% (23-66; 10/23) for Xpert and 43% (23-66; 10/23) for culture. With composite standard, we detected tuberculous meningitis in 22 (17%) of 129 participants. Xpert Ultra had 95% sensitivity (95% CI 77-99; 21 of 22 cases) for tuberculous meningitis, which was higher than either Xpert (45% [24-68]; 10/22; p=0·0010) or culture (45% [24-68]; 10/22; p=0·0034). Of 21 participants positive by Xpert Ultra, 13 were positive by culture, Xpert, or both, and eight were only positive by Xpert Ultra. Of those eight, three were categorised as probable tuberculous meningitis, three as possible tuberculous meningitis, and two as not tuberculous meningitis. Testing 6 mL or more of CSF was associated with more frequent detection of tuberculosis than with less than 6 mL (26% vs 7%; p=0·014).
Interpretation: Xpert Ultra detected significantly more tuberculous meningitis than did either Xpert or culture. WHO now recommends the use of Xpert Ultra as the initial diagnostic test for suspected tuberculous meningitis.
Funding: National Institute of Neurologic Diseases and Stroke, Fogarty International Center, National Institute of Allergy and Infectious Disease, UK Medical Research Council/DfID/Wellcome Trust Global Health Trials, Doris Duke Charitable Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Xpert MTB/RIF Ultra: a gamechanger for tuberculous meningitis?Lancet Infect Dis. 2018 Jan;18(1):6-8. doi: 10.1016/S1473-3099(17)30536-4. Epub 2017 Sep 14. Lancet Infect Dis. 2018. PMID: 28919337 No abstract available.
-
Diagnostic algorithm for low-volume CSF samples in tuberculous meningitis.Lancet Infect Dis. 2017 Dec;17(12):1236-1237. doi: 10.1016/S1473-3099(17)30639-4. Lancet Infect Dis. 2017. PMID: 29173879 No abstract available.
-
Diagnosis of tuberculous meningitis with invasive pulmonary sampling.Lancet Infect Dis. 2018 Jan;18(1):25-26. doi: 10.1016/S1473-3099(17)30713-2. Epub 2017 Dec 20. Lancet Infect Dis. 2018. PMID: 29303733 No abstract available.
-
Xpert Ultra's place in the diagnosis of tuberculous meningitis.Lancet Infect Dis. 2018 Mar;18(3):248-249. doi: 10.1016/S1473-3099(18)30091-4. Lancet Infect Dis. 2018. PMID: 29485086 No abstract available.
-
Xpert Ultra's place in the diagnosis of tuberculous meningitis - Authors' reply.Lancet Infect Dis. 2018 Mar;18(3):249-250. doi: 10.1016/S1473-3099(18)30078-1. Lancet Infect Dis. 2018. PMID: 29485087 Free PMC article. No abstract available.
References
-
- Woldeamanuel YW, Girma B. A 43-year systematic review and meta-analysis: case-fatality and risk of death among adults with tuberculous meningitis in Africa. J Neurol. 2014;261:851–865. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
