

New insight into the pathogenesis of nail psoriasis and overview of treatment strategies
- PMID: 28919705
- PMCID: PMC5587086
- DOI: 10.2147/DDDT.S136986
New insight into the pathogenesis of nail psoriasis and overview of treatment strategies
Abstract
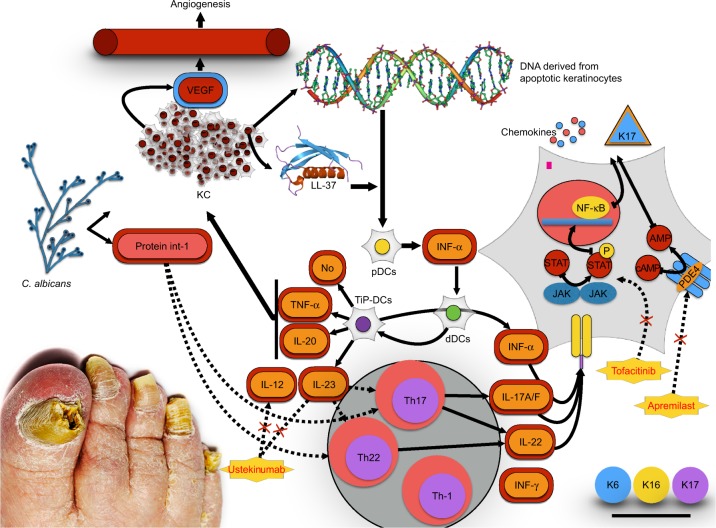
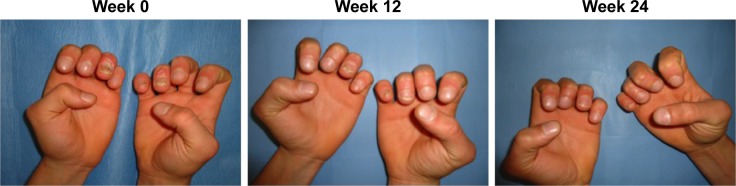
Psoriasis is a chronic inflammatory disease affecting up to 3% of the general population. The prevalence of nail involvement in psoriasis patients varies between 15% and 79%. While the nails represent a small portion of the body surface area, psoriasis in these areas can have a disproportionate influence on a patient's physical and psychosocial activities. Differential diagnosis between an onychomycosis and a psoriatic nail could be challenging; nevertheless, coexistence of onychomycosis and nail psoriasis also occurs and both are common disorders in the general population. Nail psoriasis can be difficult to treat. Treatment of nail psoriasis should consider the body surface area of skin disease, psoriatic arthritis, severity of nail disease, and the impairment in the quality of life. All patients should be tested for onychomycosis before starting a therapy. This recommendation is underlined by the fact that nail psoriasis is mostly treated by immunosuppressive drugs, like steroids, methotrexate, or biologics, which may aggravate mycotic nail infections. Conventional systemic therapy, such as use of steroids, cyclosporine, methotrexate, and retinoid in the long term, can cause organ toxicities. Currently, use of apremilast and tofacitinib favors an early healing of nail psoriasis because they act directly on the pathogenic targets, distressing the inflammatory signals associated with the initiation and maintenance of the disease activity, and as with several conventional synthetic disease modifying antirheumatic drugs, they are characterized by the convenience of oral administration. The number of treatment options has increased considerably in recent years; however, given the heterogeneity of the disease, the therapy should be personalized to individual cases.
Keywords: nail; onychomycosis; psoriasis.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Treatment of nail psoriasis: best practice recommendations from the Medical Board of the National Psoriasis Foundation.JAMA Dermatol. 2015 Jan;151(1):87-94. doi: 10.1001/jamadermatol.2014.2983. JAMA Dermatol. 2015. PMID: 25471223
-
Nail dystrophy in psoriatic arthritis presenting as nail onychomycosis: a case report.Hand Surg. 2012;17(1):139-42. doi: 10.1142/S0218810412720161. Hand Surg. 2012. PMID: 22351553
-
Nail Psoriasis.Actas Dermosifiliogr. 2022 May;113(5):481-490. doi: 10.1016/j.ad.2022.01.006. Epub 2022 Feb 2. Actas Dermosifiliogr. 2022. PMID: 35697407 Review. English, Spanish.
-
[Nail psoriasis-painful and yet undertreated : From pathogenesis to therapy].Dermatologie (Heidelb). 2025 May;76(5):267-276. doi: 10.1007/s00105-025-05495-z. Epub 2025 Apr 4. Dermatologie (Heidelb). 2025. PMID: 40183812 German.
-
Onychomycosis in patients with nail psoriasis: a point to point discussion.Mycoses. 2017 Jan;60(1):6-10. doi: 10.1111/myc.12542. Epub 2016 Aug 15. Mycoses. 2017. PMID: 27523738 Review.
Cited by
-
Fast Clinical Response of Bimekizumab in Nail Psoriasis: A Retrospective Multicenter 36-Week Real-Life Study.Pharmaceuticals (Basel). 2024 Oct 16;17(10):1378. doi: 10.3390/ph17101378. Pharmaceuticals (Basel). 2024. PMID: 39459016 Free PMC article.
-
A Real-Life Study on the Use of Tildrakizumab in Psoriatic Patients.Pharmaceuticals (Basel). 2023 Mar 31;16(4):526. doi: 10.3390/ph16040526. Pharmaceuticals (Basel). 2023. PMID: 37111283 Free PMC article.
-
Fungal Infections among Psoriatic Patients: Etiologic Agents, Comorbidities, and Vulnerable Population.Autoimmune Dis. 2021 Sep 15;2021:1174748. doi: 10.1155/2021/1174748. eCollection 2021. Autoimmune Dis. 2021. PMID: 34567800 Free PMC article.
-
Matching between ctlinical examination and dermoscopy in patients with nail psoriasis: Should dermoscopy be used instead of clinical examination?Heliyon. 2024 Apr 13;10(8):e29608. doi: 10.1016/j.heliyon.2024.e29608. eCollection 2024 Apr 30. Heliyon. 2024. PMID: 38655347 Free PMC article.
-
Successful treatment of nail psoriasis with topical roflumilast: A case report.SAGE Open Med Case Rep. 2024 Oct 22;12:2050313X241289594. doi: 10.1177/2050313X241289594. eCollection 2024. SAGE Open Med Case Rep. 2024. PMID: 39483845 Free PMC article.
References
-
- Parisi R, Symmons DP, Griffiths CE, Ashcroft DM, Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. - PubMed
-
- Gordon KB, Strober BE. Understanding therapeutic pathways and comorbidities in psoriasis. Semin Cutan Med Surg. 2014;33(2 Suppl 2):S20–S23. - PubMed
-
- Davidovici BB, Sattar N, Prinz J, et al. Psoriasis and systemic inflammatory diseases: potential mechanistic links between skin disease and co-morbid conditions. J Invest Dermatol. 2010;130(7):1785–1796. - PubMed
-
- Gottlieb AB, Dann F. Comorbidities in patients with psoriasis. Am J Med. 2009;122(12):1150.e1–e9. - PubMed
-
- Gisondi P, Ferrazzi A, Girolomoni G. Metabolic comorbidities and psoriasis. Acta Dermatovenerol Croat. 2010;18(4):297–304. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
