

Complement in cancer: untangling an intricate relationship
- PMID: 28920587
- PMCID: PMC5816344
- DOI: 10.1038/nri.2017.97
Complement in cancer: untangling an intricate relationship
Abstract
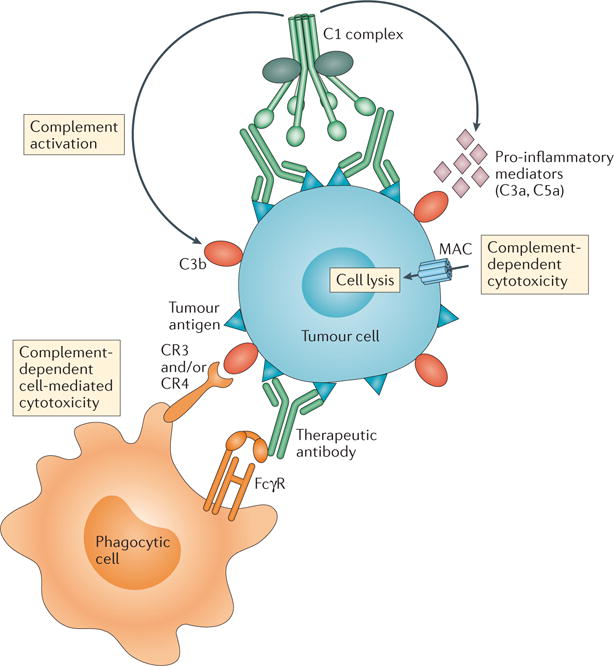
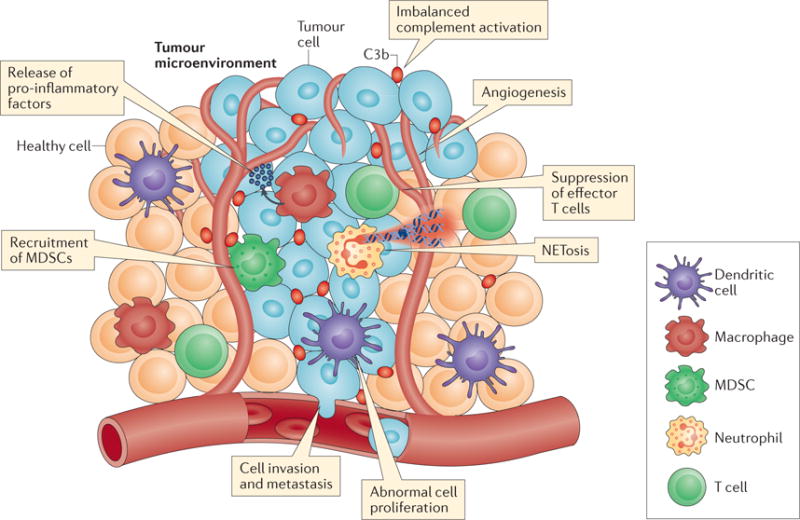
In tumour immunology, complement has traditionally been considered as an adjunctive component that enhances the cytolytic effects of antibody-based immunotherapies, such as rituximab. Remarkably, research in the past decade has uncovered novel molecular mechanisms linking imbalanced complement activation in the tumour microenvironment with inflammation and suppression of antitumour immune responses. These findings have prompted new interest in manipulating the complement system for cancer therapy. This Review summarizes our current understanding of complement-mediated effector functions in the tumour microenvironment, focusing on how complement activation can act as a negative or positive regulator of tumorigenesis. It also offers insight into clinical aspects, including the feasibility of using complement biomarkers for cancer diagnosis and the use of complement inhibitors during cancer treatment.
Conflict of interest statement
The authors declare competing interests: see Web version for details.
Figures
References
-
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454:436–444. - PubMed
-
- Chen DS, Mellman I. Elements of cancer immunity and the cancer-immune set point. Nature. 2017;541:321–330. - PubMed
-
- Berraondo P, et al. Innate immune mediators in cancer: between defense and resistance. Immunol Rev. 2016;274:290–306. - PubMed
-
- Hughes PE, Caenepeel S, Wu LC. Targeted therapy and checkpoint immunotherapy combinations for the treatment of cancer. Trends Immunol. 2016;37:462–476. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
