

Out-of-pocket expenditure and catastrophic health spending on maternal care in public and private health centres in India: a comparative study of pre and post national health mission period
- PMID: 28921477
- PMCID: PMC5603466
- DOI: 10.1186/s13561-017-0167-1
Out-of-pocket expenditure and catastrophic health spending on maternal care in public and private health centres in India: a comparative study of pre and post national health mission period
Abstract
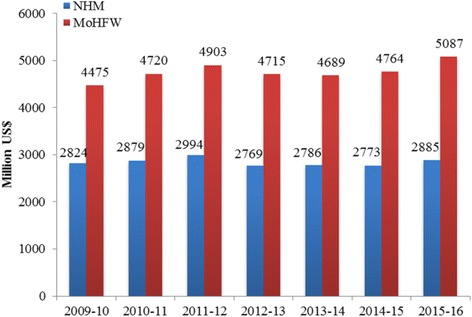
Background: The National Health Mission (NHM), one of the largest publicly funded maternal health programs worldwide was initiated in 2005 to reduce maternal, neo-natal and infant mortality and out-of-pocket expenditure (OOPE) on maternal care in India. Though evidence suggests improvement in maternal and child health, little is known on the change in OOPE and catastrophic health spending (CHS) since the launch of NHM.
Aim: The aim of this paper is to provide a comprehensive estimate of OOPE and CHS on maternal care by public and private health providers in pre and post NHM periods.
Data and method: The unit data from the 60th and 71st rounds of National Sample Survey (NSS) is used in the analyses. Descriptive statistics is used to understand the differentials in OOPE and CHS. The CHS is estimated based on capacity to pay, derived from household consumption expenditure, the subsistence expenditure (based on state specific poverty line) and household OOPE on maternal care. Data of both rounds are pooled to understand the impact of NHM on OOPE and CHS. The log-linear regression model and the logit regression models adjusted for state fixed effect, clustering and socio-economic and demographic correlates are used in the analyses.
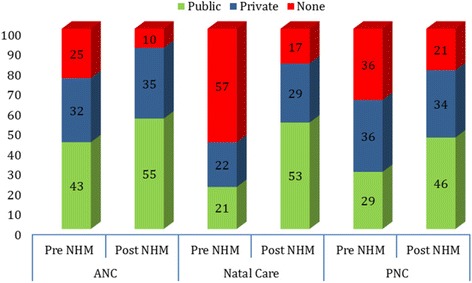
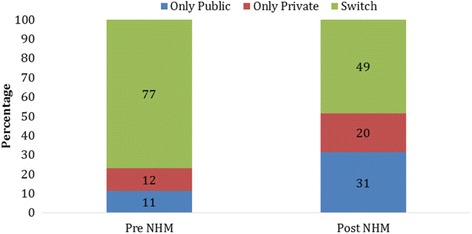
Results: Women availing themselves of ante natal, natal and post natal care (all three maternal care services) from public health centres have increased from 11% in 2004 to 31% by 2014 while that from private health centres had increased from 12% to 20% during the same period. The mean OOPE on all three maternal care services from public health centres was US$60 in pre-NHM and US$86 in post-NHM periods while that from private health center was US$170 and US$300 during the same period. Controlling for socioeconomic and demographic correlates, the OOPE on delivery care from public health center had not shown any significant increase in post NHM period. The OOPE on delivery care in private health center had increased by 5.6 times compared to that from public health centers in pre NHM period. Economic well-being of the households and educational attainment of women is positively and significantly associated with OOPE, linking OOPE and ability to pay. The extent of CHS on all three maternal care from public health centers had declined from 56% in pre NHM period to 29% in post NHM period while that from private health centres had declined from 56% to 47% during the same period. The odds of incurring CHS on institutional delivery in public health centers (OR .03, 95% CI 0.02, 06) and maternal care (OR 0.06, 95% CI 0.04, 0.07) suggest decline in CHS in the post NHM period. Women delivering in private health centres, residing in rural areas and poor households are more likely to face CHS on maternal care.
Conclusion: NHM has been successful in increasing maternal care and reducing the catastrophic health spending in public health centers. Regulating private health centres and continuing cash incentive under NHM is recommended.
Keywords: Catastrophic health spending; Delivery care; India; Maternal care; National Health Mission; National Rural Health Mission; Out-of-pocket expenditure.
Conflict of interest statement
Authors’ information
Sanjay K Mohanty is Professor at International Institute for Population Sciences, Mumbai. He has 17 years of teaching and research experience at post-graduate level. He teaches health economics and fertility at IIPS, Mumbai. His research interest includes health financing, multidimensional poverty and economics of ageing.
Anshul Kastor is doctoral student at International Institute for Population Sciences, Mumbai. He is pursuing his doctoral work on “Health financing transition and its linkages with health outcomes in India”.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- United Nations . UN sustainable goals summit 2015. New York City: United Nations; 2015. - PubMed
-
- Knaul FM, Arreola-Ornelas H, Méndez-Carniado O, Bryson-Cahn C, Barofsky J, Maguire R, Miranda M, Sesma S. Evidence is good for your health system: policy reform to remedy catastrophic and impoverishing health spending in Mexico. Lancet. 2006;368:1828–1841. doi: 10.1016/S0140-6736(06)69565-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
