

Pharmacodynamics and pharmacokinetics of ticagrelor vs. clopidogrel in patients with acute coronary syndromes and chronic kidney disease
- PMID: 28921624
- PMCID: PMC5736840
- DOI: 10.1111/bcp.13436
Pharmacodynamics and pharmacokinetics of ticagrelor vs. clopidogrel in patients with acute coronary syndromes and chronic kidney disease
Abstract
Background: Pivotal clinical trials found that ticagrelor reduced ischaemic complications to a greater extent than clopidogrel, and also that the benefit gradually increased with the reduction in creatinine clearance. However, the underlying mechanisms remains poorly explored.
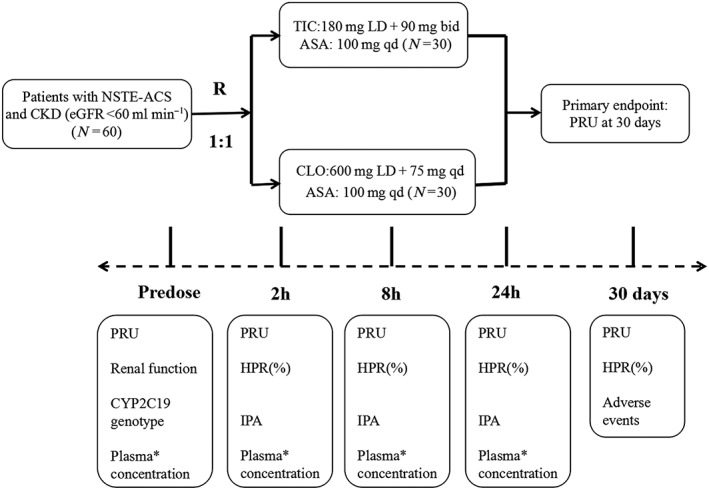
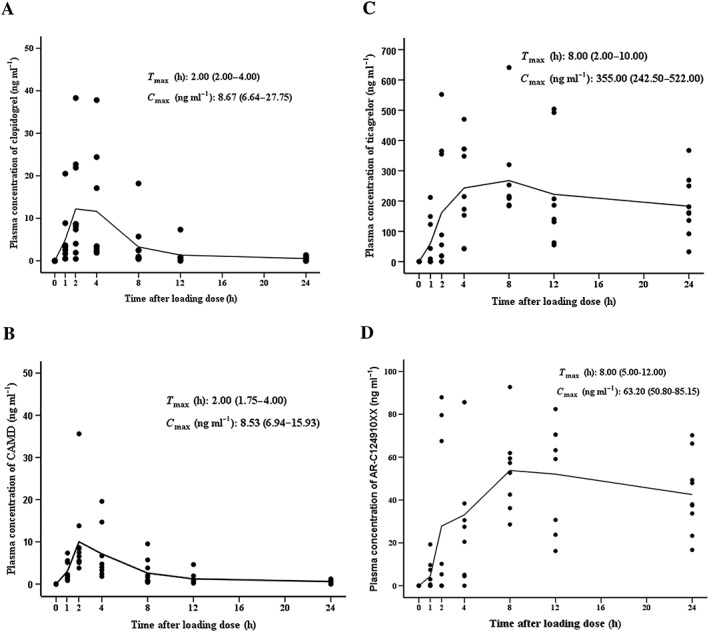
Methods: This was a single-centre, prospective, randomized clinical trial involving 60 hospitalized Adenosine Diphosphate (ADP) P2Y12 receptor inhibitor-naïve patients with chronic kidney disease (CKD) (estimated glomerular filtration rate <60 ml min-1 1.73 m-2 ) and non-ST-elevation acute coronary syndromes (NSTE-ACS). Eligible patients were randomly assigned in a 1:1 ratio to receive ticagrelor (180 mg loading dose, then followed by 90 mg twice daily) or clopidogrel (600 mg loading dose, then followed by 75 mg once daily). The primary endpoint was the P2Y12 reactive unit (PRU) value assessed by VerifyNow at 30 days. The plasma concentrations of ticagrelor and clopidogrel and their active metabolites were measured in the first 10 patients in each group at baseline, and at 1 h, 2 h, 4 h, 8 h, 12 h and 24 h after the loading dose.
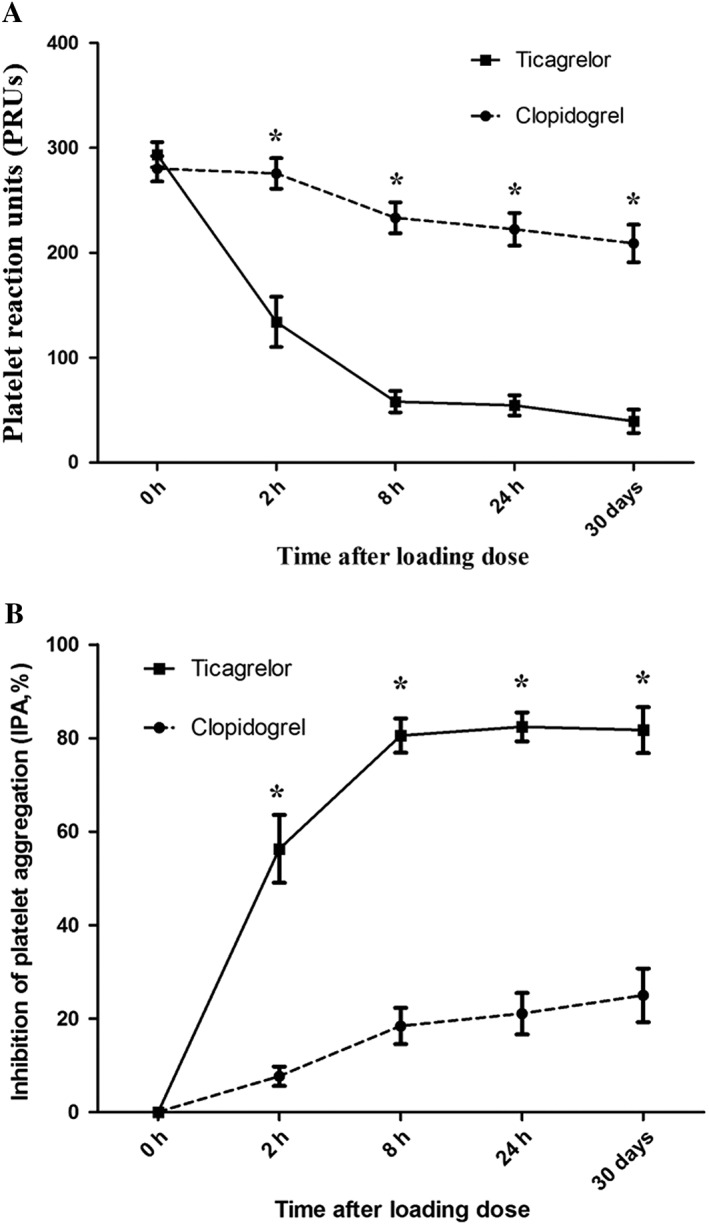
Results: Baseline characteristics were well matched between the two groups. Our results indicated a markedly lower PRU in patients treated with ticagrelor vs. clopidogrel at 30 days (32.6 ± 11.29 vs. 203.7 ± 17.92; P < 0.001) as well as at 2 h, 8 h and 24 h after the loading dose (P < 0.001). Ticagrelor and its active metabolite AR-C124910XX showed a similar time to reach maximum concentration (Cmax ) of 8 h, with the maximum concentration (Cmax ) of 355 (242.50-522.00) ng ml-1 and 63.20 (50.80-85.15) ng ml-1 , respectively. Both clopidogrel and its active metabolite approached the Cmax at 2 h, with a similar Cmax of 8.67 (6.64-27.75) ng ml-1 vs. 8.53 (6.94-15.93) ng ml-1 .
Conclusion: Ticagrelor showed much more potent platelet inhibition in comparison with clopidogrel in patients with CKD and NSTE-ACS.
Keywords: chronic kidney disease; non-ST-elevation acute coronary syndromes; pharmacodynamics; ticagrelor.
© 2017 The British Pharmacological Society.
Figures
References
-
- Best PJ, Steinhub SR, Berger PB, Dasgupta A, Brennan DM, Szczech LA, et al The efficacy and safety of short‐ and long‐term dual antiplatelet therapy in patients with mild or moderate chronic kidney disease: results from the Clopidogrel for the Reduction of Events During Observation (CREDO) trial. Am Heart J 2008; 155: 687–693. - PubMed
-
- Dasgupta A, Steinhubl SR, Bhatt DL, Berger PB, Shao M, Mak KH, et al Clinical outcomes of patients with diabetic nephropathy randomized to clopidogrel plus aspirin versus aspirin alone (a post hoc analysis of the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance [CHARISMA] trial). Am J Cardiol 2009; 103: 1359–1363. - PubMed
-
- Park SH, Kim W, Park CS, Kang WY, Hwang SH, Kim W. A comparison of clopidogrel responsiveness in patients with versus without chronic renal failure. Am J Cardiol 2009; 104: 1292–1295. - PubMed
-
- Angiolillo DJ, Bernardo E, Capodanno D, Vivas D, Sabaté M, Ferreiro JL, et al Impact of chronic kidney disease on platelet function profiles in diabetes mellitus patients with coronary artery disease taking dual antiplatelet therapy. J Am Coll Cardiol 2010; 55: 1139–1146. - PubMed
-
- Guo LZ, Kim MH, Shim CH, Choi SY, Serebruany VL. Impact of renal impairment on platelet reactivity and clinical outcomes during chronic dual antiplatelet therapy following coronary stenting. Eur Heart J Cardiovasc Pharmacother 2016; 2: 145–151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
