

Validation of highly accelerated real-time cardiac cine MRI with radial k-space sampling and compressed sensing in patients at 1.5T and 3T
- PMID: 28921631
- PMCID: PMC5821536
- DOI: 10.1002/mrm.26918
Validation of highly accelerated real-time cardiac cine MRI with radial k-space sampling and compressed sensing in patients at 1.5T and 3T
Abstract
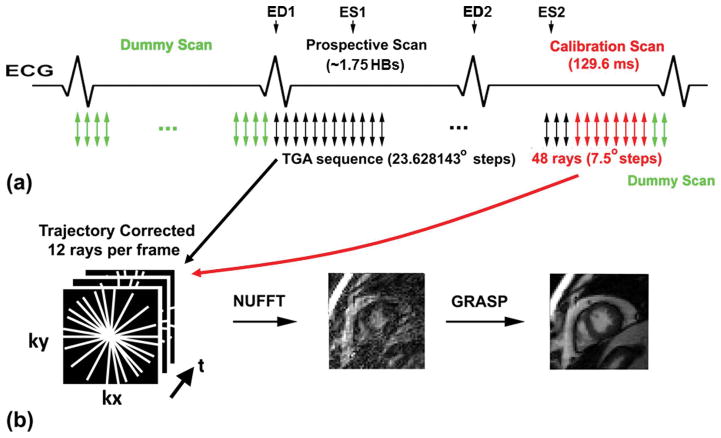
Purpose: To validate an optimal 12-fold accelerated real-time cine MRI pulse sequence with radial k-space sampling and compressed sensing (CS) in patients at 1.5T and 3T.
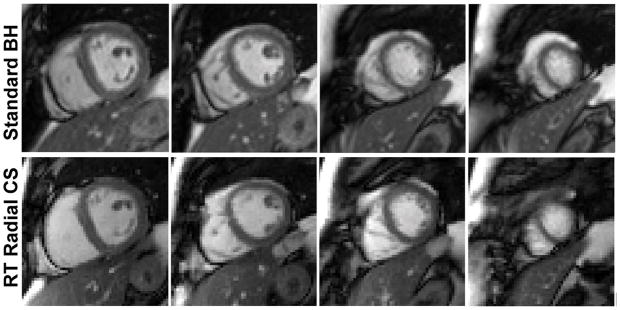
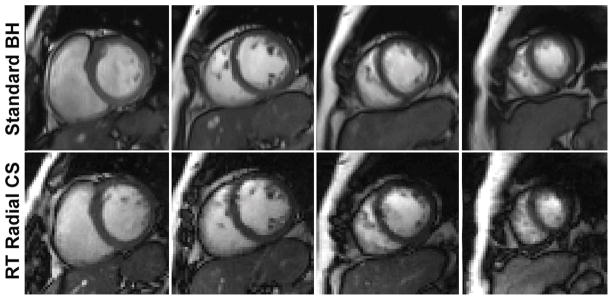
Methods: We used two strategies to reduce image artifacts arising from gradient delays and eddy currents in radial k-space sampling with balanced steady-state free precession readout. We validated this pulse sequence against a standard breath-hold cine sequence in two patient cohorts: a myocardial infarction (n = 16) group at 1.5T and chronic kidney disease group (n = 18) at 3T. Two readers independently performed visual analysis of 68 cine sets in four categories (myocardial definition, temporal fidelity, artifact, noise) on a 5-point Likert scale (1 = nondiagnostic, 2 = poor, 3 = adequate or moderate, 4 = good, 5 = excellent). Another reader calculated left ventricular (LV) functional parameters, including ejection fraction.
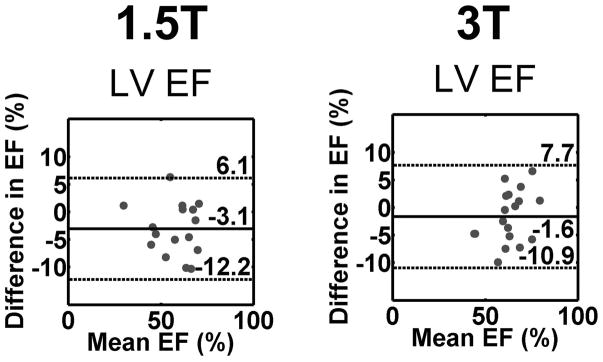
Results: Compared with standard cine, real-time cine produced nonsignificantly different visually assessed scores, except for the following categories: 1) temporal fidelity scores were significantly lower (P = 0.013) for real-time cine at both field strengths, 2) artifacts scores were significantly higher (P = 0.013) for real-time cine at both field strengths, and 3) noise scores were significantly (P = 0.013) higher for real-time cine at 1.5T. Standard and real-time cine pulse sequences produced LV functional parameters that were in good agreement (e.g., absolute mean difference in ejection fraction <4%).
Conclusion: This study demonstrates that an optimal 12-fold, accelerated, real-time cine MRI pulse sequence using radial k-space sampling and CS produces good to excellent visual scores and relatively accurate LV functional parameters in patients at 1.5T and 3T. Magn Reson Med 79:2745-2751, 2018. © 2017 International Society for Magnetic Resonance in Medicine.
Keywords: Cartesian k-space; cardiac function; compressed sensing; radial k-space; real-time cine MRI; tiny golden angles.
© 2017 International Society for Magnetic Resonance in Medicine.
Figures
References
-
- Carr JC, Simonetti O, Bundy J, Li D, Pereles S, Finn JP. Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology. 2001;219(3):828–34. - PubMed
-
- Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, Friedrich MG, Ho VB, Jerosch-Herold M, Kramer CM, Manning WJ, Patel M, Pohost GM, Stillman AE, White RD, Woodard PK. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. 2010;55(23):2614–62. - PMC - PubMed
-
- Barkhausen J, Goyen M, Ruhm SG, Eggebrecht H, Debatin JF, Ladd ME. Assessment of ventricular function with single breath-hold real-time steady-state free precession cine MR imaging. AJR Am J Roentgenol. 2002;178(3):731–5. - PubMed
-
- Kellman P, Chefd’hotel C, Lorenz CH, Mancini C, Arai AE, McVeigh ER. Fully automatic, retrospective enhancement of real-time acquired cardiac cine MR images using image-based navigators and respiratory motion-corrected averaging. Magn Reson Med. 2008;59(4):771–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
