

Pharmacogenomics Implementation at the National Institutes of Health Clinical Center
- PMID: 28921647
- PMCID: PMC5657584
- DOI: 10.1002/jcph.993
Pharmacogenomics Implementation at the National Institutes of Health Clinical Center
Abstract
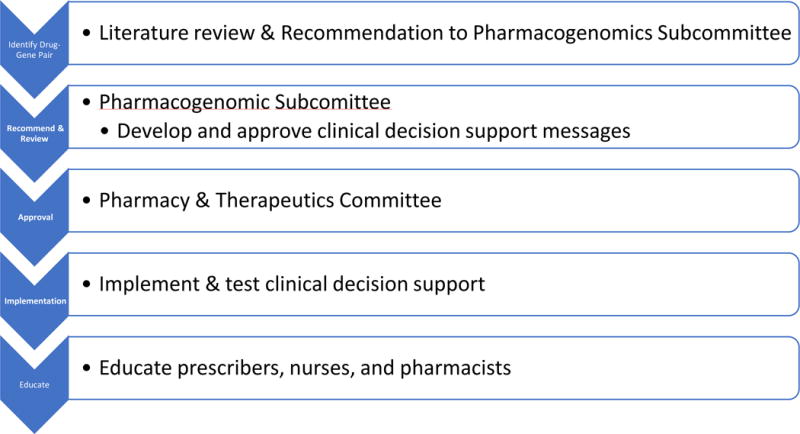
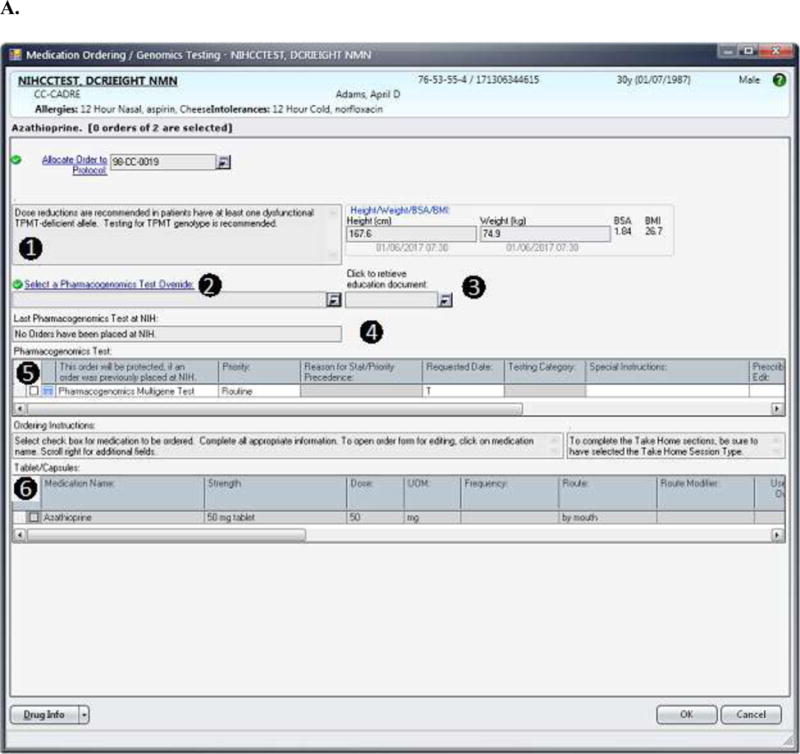
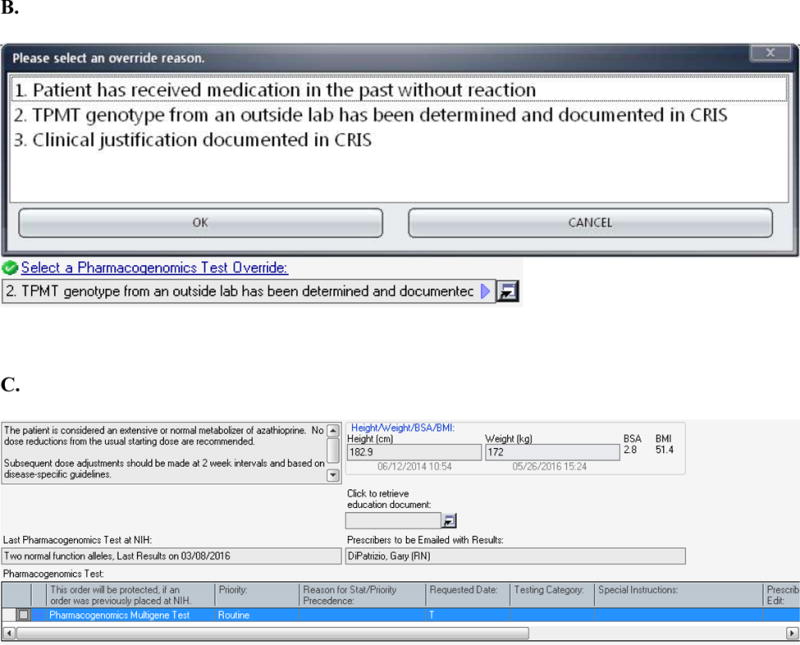
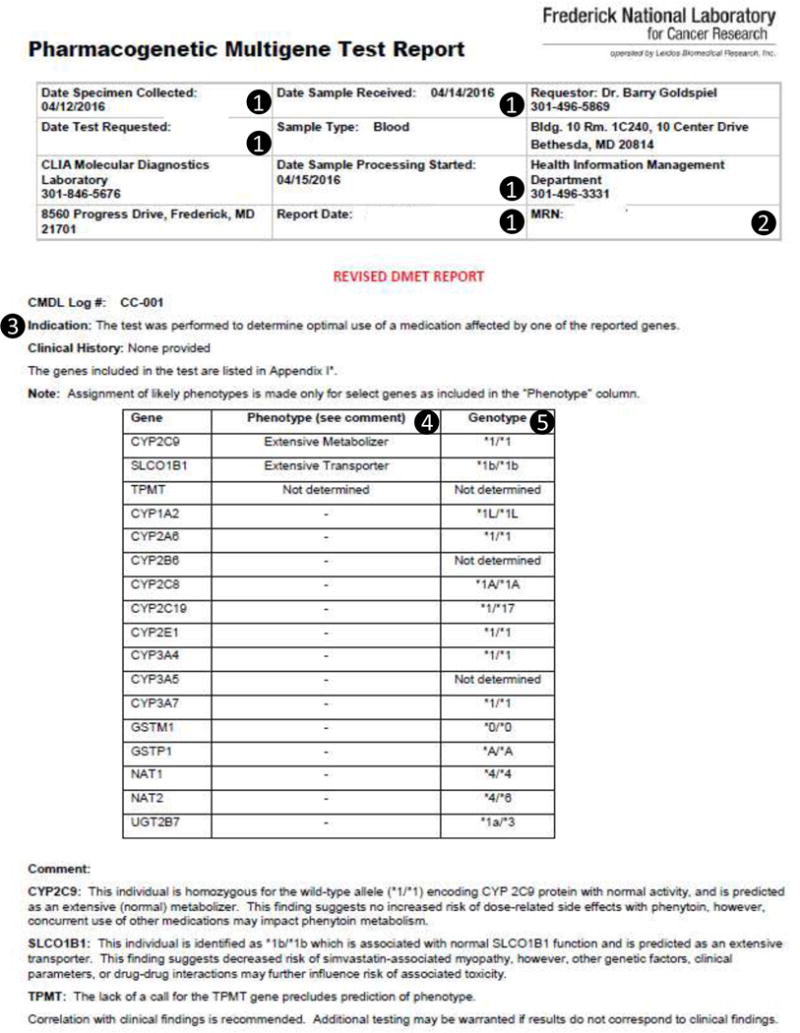
The National Institutes of Health Clinical Center (NIH CC) is the largest hospital in the United States devoted entirely to clinical research, with a highly diverse spectrum of patients. Patient safety and clinical quality are major goals of the hospital, and therapy is often complicated by multiple cotherapies and comorbidities. To this end, we implemented a pharmacogenomics program in 2 phases. In the first phase, we implemented genotyping for HLA-A and HLA-B gene variations with clinical decision support (CDS) for abacavir, carbamazepine, and allopurinol. In the second phase, we implemented genotyping for drug-metabolizing enzymes and transporters: SLCO1B1 for CDS of simvastatin and TPMT for CDS of mercaptopurine, azathioprine, and thioguanine. The purpose of this review is to describe the implementation process, which involves clinical, laboratory, informatics, and policy decisions pertinent to the NIH CC.
Keywords: implementation; pharmacogenomics; precision medicine; translation.
© 2017, The American College of Clinical Pharmacology.
Figures
References
-
- Kaniwa N, Saito Y. Pharmacogenomics of severe cutaneous adverse reactions and drug-induced liver injury. J Hum Genet. 2013;58(6):317–326. - PubMed
-
- Teh LK, Bertilsson L. Pharmacogenomics of CYP2D6: molecular genetics, interethnic differences and clinical importance. Drug Metab Pharmacokinet. 2012;27(1):55–67. - PubMed
-
- Khorasani R, Hentel K, Darer J, et al. Ten commandments for effective clinical decision support for imaging: enabling evidence-based practice to improve quality and reduce waste. AJR Am J Roentgenol. 2014;203(5):945–951. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
