

Detecting and confirming residual hotspots of lymphatic filariasis transmission in American Samoa 8 years after stopping mass drug administration
- PMID: 28922418
- PMCID: PMC5619835
- DOI: 10.1371/journal.pntd.0005914
Detecting and confirming residual hotspots of lymphatic filariasis transmission in American Samoa 8 years after stopping mass drug administration
Abstract
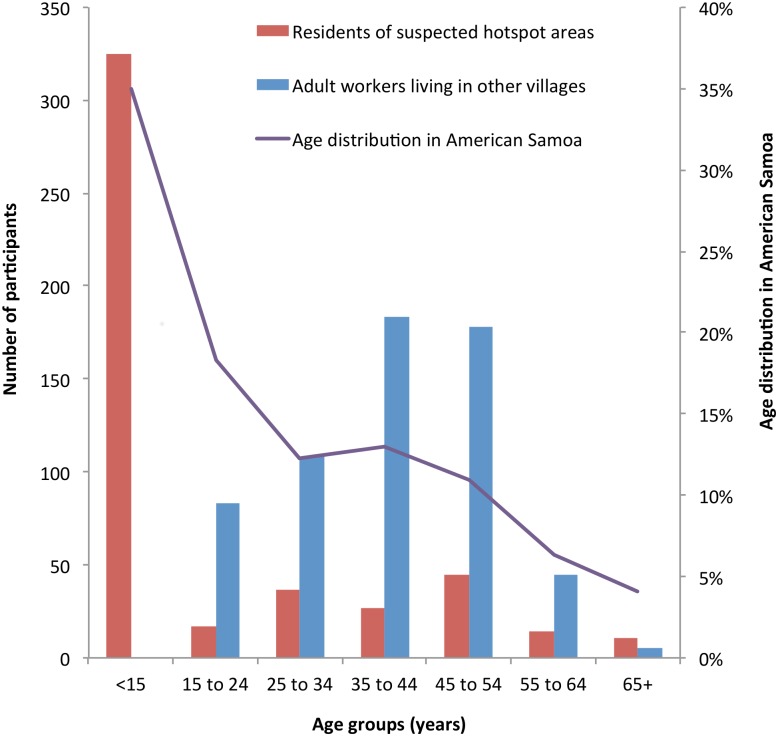
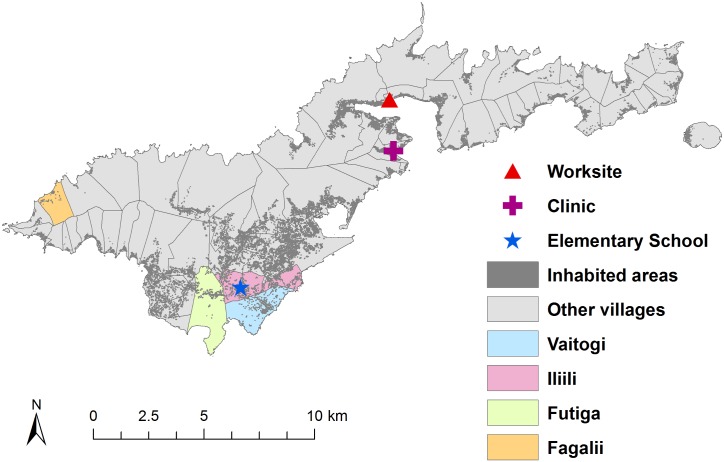
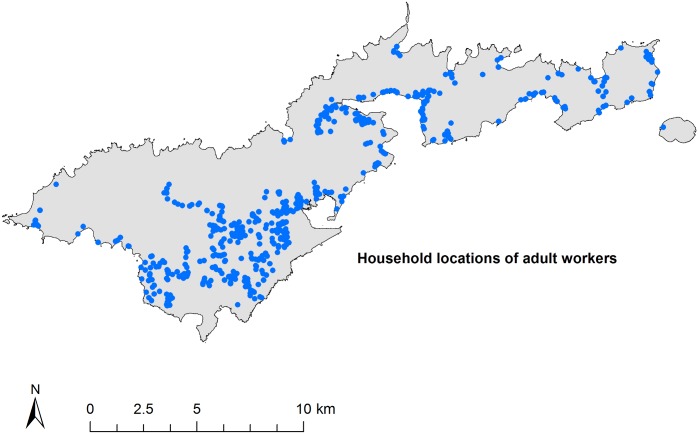
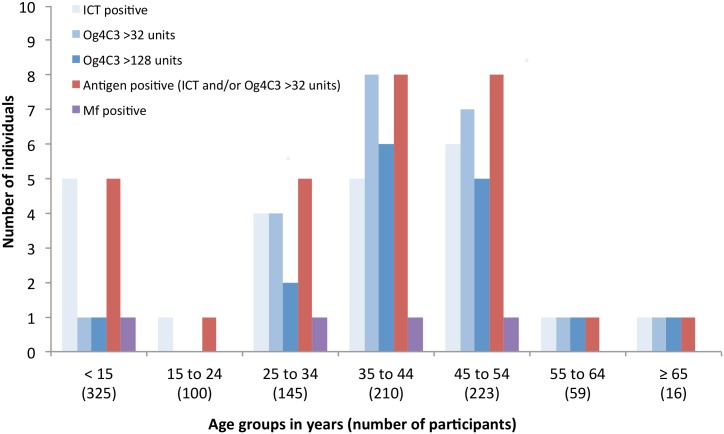
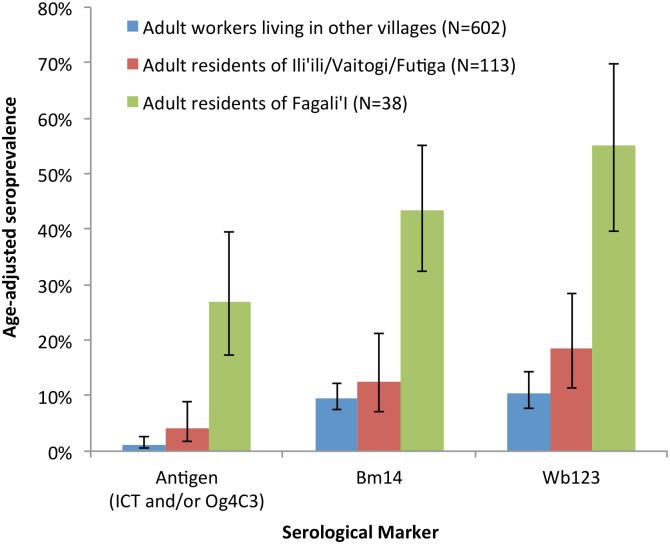
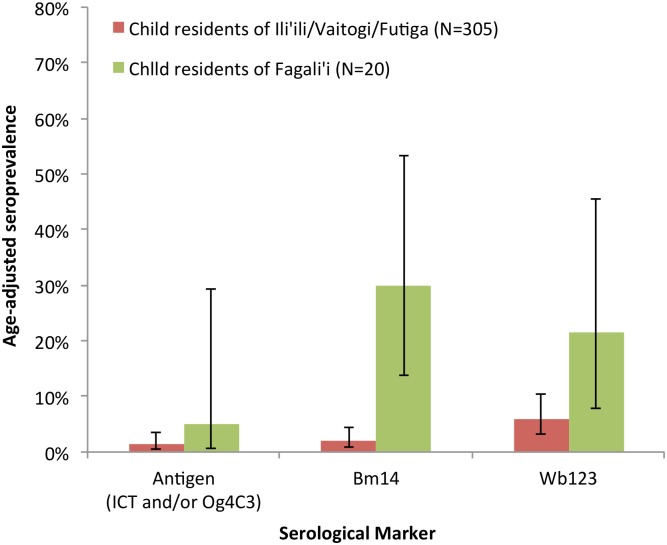
The Global Programme to Eliminate Lymphatic Filariasis (LF) aims to eliminate the disease as a public health problem by 2020 by conducting mass drug administration (MDA) and controlling morbidity. Once elimination targets have been reached, surveillance is critical for ensuring that programmatic gains are sustained, and challenges include timely identification of residual areas of transmission. WHO guidelines encourage cost-efficient surveillance, such as integration with other population-based surveys. In American Samoa, where LF is caused by Wuchereria bancrofti, and Aedes polynesiensis is the main vector, the LF elimination program has made significant progress. Seven rounds of MDA (albendazole and diethycarbamazine) were completed from 2000 to 2006, and Transmission Assessment Surveys were passed in 2010/2011 and 2015. However, a seroprevalence study using an adult serum bank collected in 2010 detected two potential residual foci of transmission, with Og4C3 antigen (Ag) prevalence of 30.8% and 15.6%. We conducted a follow up study in 2014 to verify if transmission was truly occurring by comparing seroprevalence between residents of suspected hotspots and residents of other villages. In adults from non-hotspot villages (N = 602), seroprevalence of Ag (ICT or Og4C3), Bm14 antibody (Ab) and Wb123 Ab were 1.2% (95% CI 0.6-2.6%), 9.6% (95% CI 7.5%-12.3%), and 10.5% (95% CI 7.6-14.3%), respectively. Comparatively, adult residents of Fagali'i (N = 38) had significantly higher seroprevalence of Ag (26.9%, 95% CI 17.3-39.4%), Bm14 Ab (43.4%, 95% CI 32.4-55.0%), and Wb123 Ab 55.2% (95% CI 39.6-69.8%). Adult residents of Ili'ili/Vaitogi/Futiga (N = 113) also had higher prevalence of Ag and Ab, but differences were not statistically significant. The presence of transmission was demonstrated by 1.1% Ag prevalence (95% CI 0.2% to 3.1%) in 283 children aged 7-13 years who lived in one of the suspected hotspots; and microfilaraemia in four individuals, all of whom lived in the suspected hotspots, including a 9 year old child. Our results provide field evidence that integrating LF surveillance with other surveys is effective and feasible for identifying potential hotspots, and conducting surveillance at worksites provides an efficient method of sampling large populations of adults.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Lymphatic Filariasis Elimination in American Samoa: Evaluation of Molecular Xenomonitoring as a Surveillance Tool in the Endgame.PLoS Negl Trop Dis. 2016 Nov 1;10(11):e0005108. doi: 10.1371/journal.pntd.0005108. eCollection 2016 Nov. PLoS Negl Trop Dis. 2016. PMID: 27802280 Free PMC article.
-
Seroprevalence and spatial epidemiology of Lymphatic Filariasis in American Samoa after successful mass drug administration.PLoS Negl Trop Dis. 2014 Nov 13;8(11):e3297. doi: 10.1371/journal.pntd.0003297. eCollection 2014. PLoS Negl Trop Dis. 2014. PMID: 25393716 Free PMC article.
-
Potential strategies for strengthening surveillance of lymphatic filariasis in American Samoa after mass drug administration: Reducing 'number needed to test' by targeting older age groups, hotspots, and household members of infected persons.PLoS Negl Trop Dis. 2020 Dec 28;14(12):e0008916. doi: 10.1371/journal.pntd.0008916. eCollection 2020 Dec. PLoS Negl Trop Dis. 2020. PMID: 33370264 Free PMC article.
-
Control and elimination of lymphatic filariasis in Oceania: Prevalence, geographical distribution, mass drug administration, and surveillance in Samoa, 1998-2017.Adv Parasitol. 2021;114:27-73. doi: 10.1016/bs.apar.2021.03.002. Epub 2021 Aug 9. Adv Parasitol. 2021. PMID: 34696844 Review.
-
Albendazole alone or in combination with microfilaricidal drugs for lymphatic filariasis.Cochrane Database Syst Rev. 2019 Jan 8;1(1):CD003753. doi: 10.1002/14651858.CD003753.pub4. Cochrane Database Syst Rev. 2019. PMID: 30620051 Free PMC article.
Cited by
-
The History of Bancroftian Lymphatic Filariasis in Australasia and Oceania: Is There a Threat of Re-Occurrence in Mainland Australia?Trop Med Infect Dis. 2018 Jun 4;3(2):58. doi: 10.3390/tropicalmed3020058. Trop Med Infect Dis. 2018. PMID: 30274454 Free PMC article. Review.
-
Positive-case follow up for lymphatic filariasis after a transmission assessment survey in Haiti.PLoS Negl Trop Dis. 2022 Feb 25;16(2):e0010231. doi: 10.1371/journal.pntd.0010231. eCollection 2022 Feb. PLoS Negl Trop Dis. 2022. PMID: 35213537 Free PMC article.
-
Post-Treatment Surveillance for Lymphatic Filariasis in Plateau and Nasarawa States, Nigeria: Results of Transmission Assessment Surveys.Am J Trop Med Hyg. 2020 Jun;102(6):1404-1410. doi: 10.4269/ajtmh.20-0020. Am J Trop Med Hyg. 2020. PMID: 32228796 Free PMC article.
-
New distribution patterns of Dirofilaria immitis in Italy.Front Vet Sci. 2023 May 4;10:1162403. doi: 10.3389/fvets.2023.1162403. eCollection 2023. Front Vet Sci. 2023. PMID: 37215465 Free PMC article.
-
Spatiotemporal Dynamics of Sporadic Shiga Toxin-Producing Escherichia coli Enteritis, Ireland, 2013-2017.Emerg Infect Dis. 2021 Sep;27(9):2421-2433. doi: 10.3201/eid2709.204021. Emerg Infect Dis. 2021. PMID: 34424163 Free PMC article.
References
-
- Ramaiah KD, Ottesen EA. Progress and Impact of 13 Years of the Global Programme to Eliminate Lymphatic Filariasis on Reducing the Burden of Filarial Disease. PLoS Negl Trop Dis. 2014;8:e3319 doi: 10.1371/journal.pntd.0003319 - DOI - PMC - PubMed
-
- Global Programme to Eliminate Lymphatic Filariasis: Progress Report, 2015. Wkly Epidemiol Rec. 2016;91:441–455. - PubMed
-
- Ichimori K, Crump A. Pacific Collaboration to Eliminate Lymphatic Filariasis. Trends in Parasitology. 2005;21:441–444. doi: 10.1016/j.pt.2005.08.010 - DOI - PMC - PubMed
-
- World Health Organization. The PacELF Way: Towards the Elimination of Lymphatic Filariasis from the Pacific, 1999–2005. 1st ed Manila: WHO Regional Office for the Western Pacific; 2006.
-
- World Health Organization. Lymphatic Filariasis—Research. 2016. http://www.who.int/lymphatic_filariasis/research/en/
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
