

The association of sleep disordered breathing with left ventricular remodeling in CAD patients: a cross-sectional study
- PMID: 28923022
- PMCID: PMC5604350
- DOI: 10.1186/s12872-017-0684-1
The association of sleep disordered breathing with left ventricular remodeling in CAD patients: a cross-sectional study
Abstract
Background: There is still insufficient knowledge on the potential effect of mild to moderate sleep-disordered breathing (SDB) that is widely prevalent, often asymptomatic, and largely undiagnosed in patients with stable coronary artery disease (CAD). SDB affects 34% of men and 17% of women aged between 30 and 70. The objective of this study was to evaluate the association between SDB and left ventricular (LV) hypertrophy as well as structural remodeling in stable CAD patients.
Methods: The study was based on a cross-sectional design. Echocardiography and polysomnography was performed in 772 patients with CAD and with untreated sleep apnea. All study participants underwent testing by Epworth Sleepiness Scale questionnaire. Their mean age, NYHA and left ventricular ejection fraction were, respectively: 57 ± 9 years, 2.1 ± 0.5 and 51 ± 8%, and 76% were men. Sleep apnea (SA) was defined as an apnea-hypopnea-index (AHI) ≥5 events/h, and, non-SA, as an AHI <5.
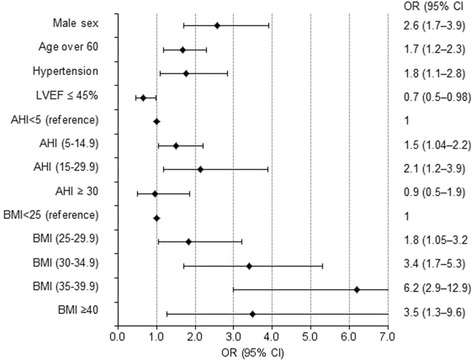
Results: Sleep apnea was present in 39% of patients, and a large fraction of those patients had no complaints on excessive daytime sleepiness. The patients with SA were older, with higher body mass and higher prevalence of hypertension. LV hypertrophy (LVH), defined by allometrically corrected (LV mass/height2.7) gender-independent criteria, was more common among the patients with SA than those without (86% vs. 74%, p < 0.001). The frequency of LVH by wall thickness criteria (interventricular septal thickness or posterior wall thickness ≥ 12 mm: 49% vs. 33%, p < 0.001) and concentric LVH (61% vs. 47%, p = 0.001) was higher in CAD patients with SA. The patients with SA had significantly higher values of both interventricular septal thickness and posterior wall thickness. Multiple logistic regression analysis showed that even mild sleep apnea was an independent predictor for LVH by wall thickness criteria and concentric LVH (OR = 1.5; 95% CI 1.04-2.2 and OR = 1.9; 1.3-2.9 respectively).
Conclusions: We concluded that unrecognized sleep apnea was highly prevalent among patients with stable CAD, and the majority of those patients did not report daytime sleepiness. Mild to moderate sleep apnea was associated with increased LV wall thickness, LV mass, and with higher prevalence of concentric LV hypertrophy independently of coexisting obesity, hypertension, diabetes mellitus or advancing age.
Keywords: Cad; Echocardiography; Hypertrophy; Left ventricular geometry; Polysomnography; Sleep apnea.
Conflict of interest statement
Ethics approval and consent to participate
The study and its consent procedures were approved by the Lithuanian Bioethics Committee (Certificate No. BE-2-21 issued at 2007–04-13) and conform to the ethical guidelines of the 2000 Declaration of Helsinki. Written informed consent was obtained from each study patient.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Somers VK, White DP, Amin R. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation scientific statement from the American Heart Association Council for high blood pressure research professional education committee, council on clinical cardiology, stroke council, and council on cardiovascular nursing. Circulation. 2008;118:1080–1111. - PubMed
-
- Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. 2009;373(9657):82–93. doi:10.1016/S0140-6736(08)61622-0. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
