

Hypothermia for encephalopathy in low and middle-income countries (HELIX): study protocol for a randomised controlled trial
- PMID: 28923118
- PMCID: PMC5604260
- DOI: 10.1186/s13063-017-2165-3
Hypothermia for encephalopathy in low and middle-income countries (HELIX): study protocol for a randomised controlled trial
Abstract
Background: Therapeutic hypothermia reduces death and disability after moderate or severe neonatal encephalopathy in high-income countries and is used as standard therapy in these settings. However, the safety and efficacy of cooling therapy in low- and middle-income countries (LMICs), where 99% of the disease burden occurs, remains unclear. We will examine whether whole body cooling reduces death or neurodisability at 18-22 months after neonatal encephalopathy, in LMICs.
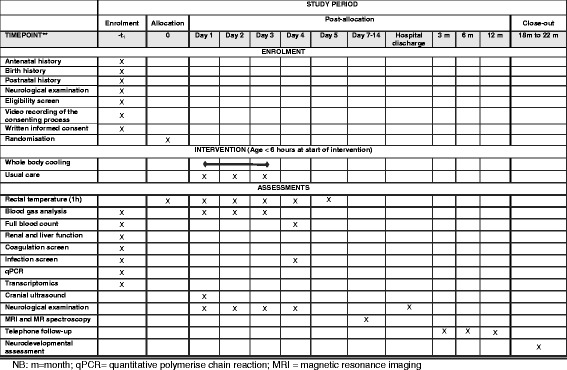
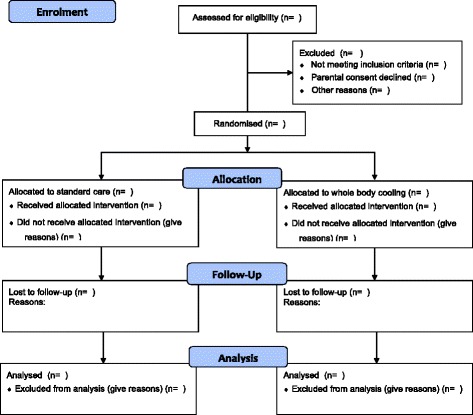
Methods: We will randomly allocate 408 term or near-term babies (aged ≤ 6 h) with moderate or severe neonatal encephalopathy admitted to public sector neonatal units in LMIC countries (India, Bangladesh or Sri Lanka), to either usual care alone or whole-body cooling with usual care. Babies allocated to the cooling arm will have core body temperature maintained at 33.5 °C using a servo-controlled cooling device for 72 h, followed by re-warming at 0.5 °C per hour. All babies will have detailed infection screening at the time of recruitment and 3 Telsa cerebral magnetic resonance imaging and spectroscopy at 1-2 weeks after birth. Our primary endpoint is death or moderate or severe disability at the age of 18 months.
Discussion: Upon completion, HELIX will be the largest cooling trial in neonatal encephalopathy and will provide a definitive answer regarding the safety and efficacy of cooling therapy for neonatal encephalopathy in LMICs. The trial will also provide important data about the influence of co-existent perinatal infection on the efficacy of hypothermic neuroprotection.
Trial registration: ClinicalTrials.gov, NCT02387385 . Registered on 27 February 2015.
Conflict of interest statement
Ethics approval and consent to participate
Imperial College Research Ethics Committee (Central Ethics Committee for the HELIX trial) has approved the trial (ICREC Reference 15IC2564; 20 April 2015). The REC approvals at the following recruiting centres have already been obtained: Calicut Medical College, Kerala, India (IRC/2015/Protocol/57; 12 June 2015); Indira Gandhi Institute of Child Health, Bangalore, India (IEC01062015; 1 June 2015); Lokmanya Tilak Municipal Medical College staff and research society (IEC/30/15; 17 June 2015); Madras Medical College Institutional Ethics Committee (IEC08072015; 7 July 2015); Maulana Azad Medical College Institutional Ethics Committee (IEC/MAMC/52/1/2016; 30 March 2016); Bangabandhu Sheikh Mujib Medical University Institutional Review Board (BSMMU/2016/6885; 29 June 2016); and Ethics Review Committee, University of Kelaniya (P/109/03/2017; 3 April 2017) (Table 3). The Health Ministry’s Screening Committee (HMSC) of India and the Indian Council of Medical Research (ICMR) have also approved the proposal. All original trial documentation and any subsequent amendments will be approved by the Sponsor (Imperial College London) and by the relevant ethical bodies, before their implementation. Informed written parental consent will be obtained from parents of next kin of recruited babies and the consenting process will be video-recorded.
Consent for publication
Written informed consent was obtained from the parents for publication of their individual details and any accompanying images in this manuscript. The consent form is held by the authors and in the patients’ clinical notes and is available for review by the Editor-in-Chief.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Pierrat VHN, Liska A, Thomas D, Subtil D, Truffert P, Groupe d’Etudes en Epidemiologie Perinatale Prevalence, causes, and outcome at 2 years of age of newborn encephalopathy: population based study. Arch Dis Child Fetal Neonatal Ed. 2005;90(3):F257–F261. doi: 10.1136/adc.2003.047985. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
