

Variations in infant and childhood vitamin D supplementation programmes across Europe and factors influencing adherence
- PMID: 28924002
- PMCID: PMC5655685
- DOI: 10.1530/EC-17-0193
Variations in infant and childhood vitamin D supplementation programmes across Europe and factors influencing adherence
Abstract
Background: Nutritional rickets is a growing global public health concern despite existing prevention programmes and health policies. We aimed to compare infant and childhood vitamin D supplementation policies, implementation strategies and practices across Europe and explore factors influencing adherence.
Methods: European Society for Paediatric Endocrinology Bone and Growth Plate Working Group members and other specialists completed a questionnaire on country-specific vitamin D supplementation policy and child health care programmes, socioeconomic factors, policy implementation strategies and adherence. Factors influencing adherence were assessed using Kendall's tau-b correlation coefficient.
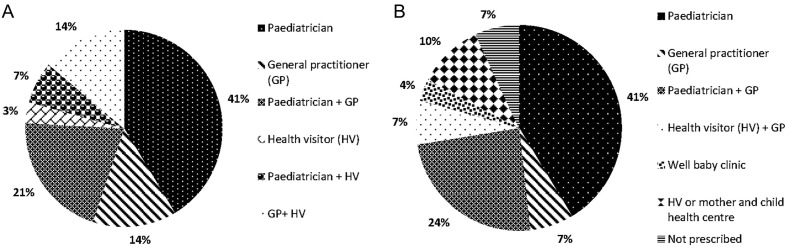
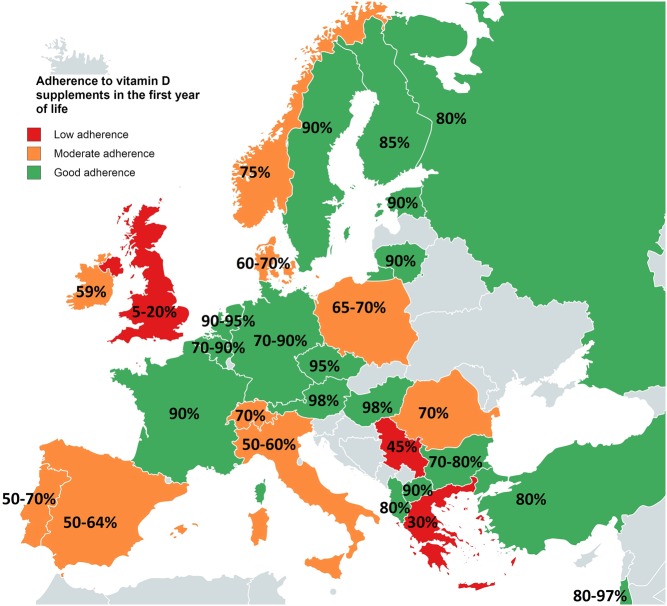
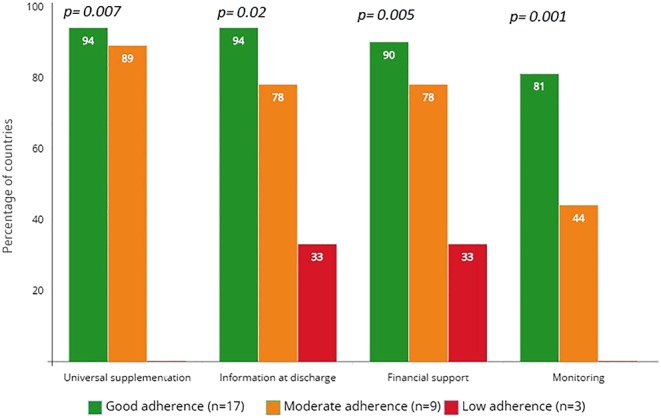
Results: Responses were received from 29 of 30 European countries (97%). Ninety-six per cent had national policies for infant vitamin D supplementation. Supplements are commenced on day 1-5 in 48% (14/29) of countries, day 6-21 in 48% (14/29); only the UK (1/29) starts supplements at 6 months. Duration of supplementation varied widely (6 months to lifelong in at-risk populations). Good (≥80% of infants), moderate (50-79%) and low adherence (<50%) to supplements was reported by 59% (17/29), 31% (9/29) and 10% (3/29) of countries, respectively. UK reported lowest adherence (5-20%). Factors significantly associated with good adherence were universal supplementation independent of feeding mode (P = 0.007), providing information at neonatal unit (NNU) discharge (P = 0.02), financial family support (P = 0.005); monitoring adherence at surveillance visits (P = 0.001) and the total number of factors adopted (P < 0.001).
Conclusions: Good adherence to supplementation is a multi-task operation that works best when parents are informed at birth, all babies are supplemented, and adherence monitoring is incorporated into child health surveillance visits. Implementation strategies matter for delivering efficient prevention policies.
Keywords: Europe; fortification; micronutrients; policy implementation; rickets; supplementation.
© 2017 The authors.
Figures
References
-
- Holick MF. Vitamin D deficiency. New England Journal of Medicine 2007. 357 266–281. - PubMed
-
- Munns CF, Shaw N, Kiely M, Specker BL, Thacher TD, Ozono K, Michigami T, Tiosano D, Mughal MZ, Mäkitie O, et al. Global consensus recommendations on prevention and management of nutritional rickets. Journal of Clinical Endocrinology and Metabolism 2016. 101 394–415. (10.1210/jc.2015-2175) - DOI - PMC - PubMed
-
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific opinion on the substantiation of a health claim related to vitamin D and contribution to normal bone and tooth development pursuant to Article 14 of Regulation (EC) No 1924/2006. EFSA Journal 2014. 12 3579 (10.2903/j.efsa.2014.3579) - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
