

Kinetics and biomarkers of severe cytokine release syndrome after CD19 chimeric antigen receptor-modified T-cell therapy
- PMID: 28924019
- PMCID: PMC5701525
- DOI: 10.1182/blood-2017-06-793141
Kinetics and biomarkers of severe cytokine release syndrome after CD19 chimeric antigen receptor-modified T-cell therapy
Abstract
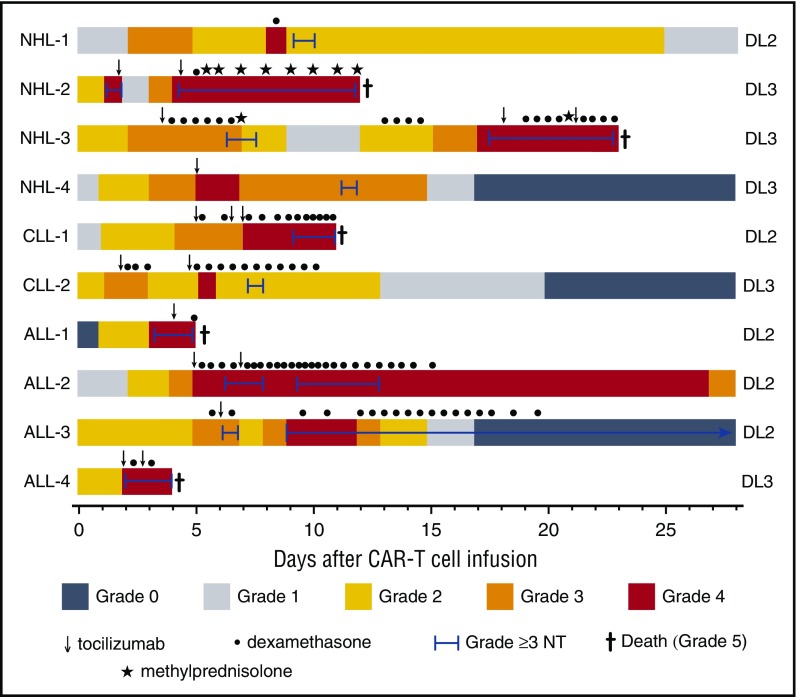
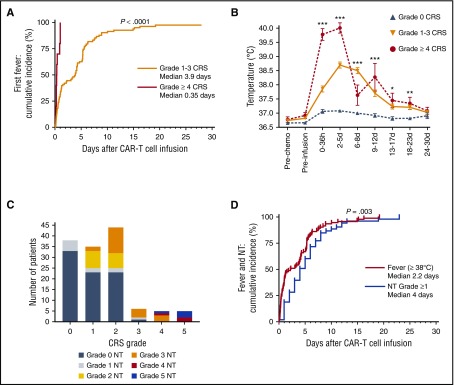
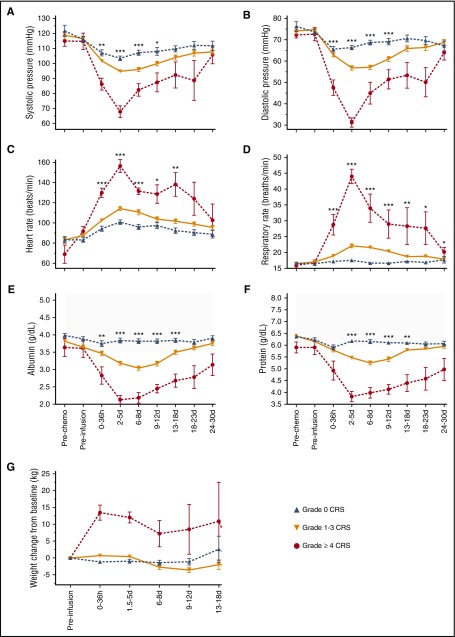
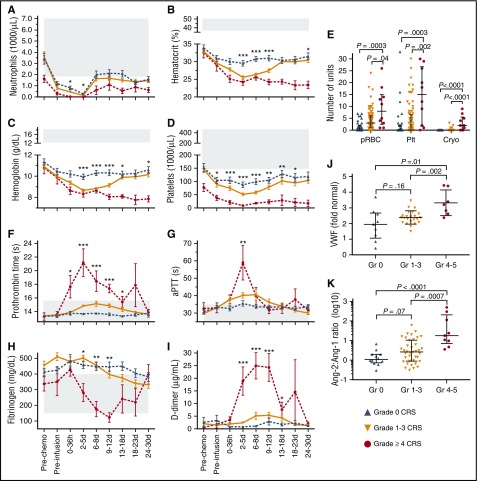
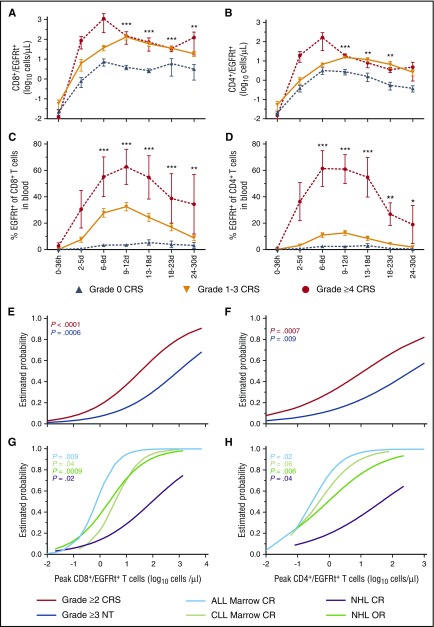
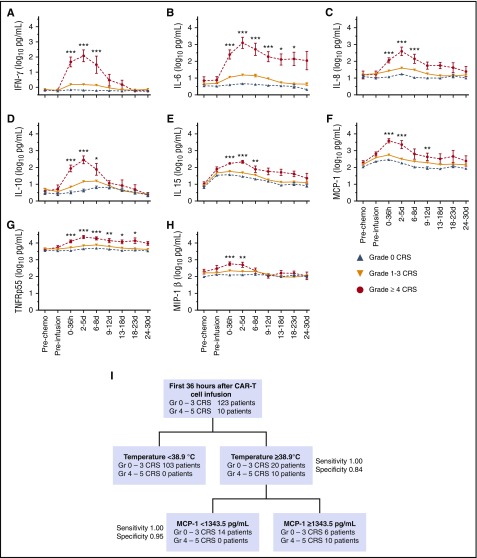
Lymphodepletion chemotherapy followed by infusion of CD19-specific chimeric antigen receptor-modified (CAR) T cells has produced impressive antitumor responses in patients with refractory CD19+ B-cell malignancies but is often associated with cytokine release syndrome (CRS). Our understanding of CRS continues to evolve, and identification of the kinetics of CRS and predictive clinical and laboratory biomarkers of severity are needed to evaluate strategies to mitigate toxicity. We report the clinical presentation of and identify biomarkers of severe CRS in 133 adult patients who received CD19 CAR T cells. CRS developed in 70% of patients, including 62.5% with grade 1 to 3 CRS (grade 1, 26%; grade 2, 32%; grade 3, 4.5%), 3.8% with grade 4, and 3.8% with grade 5. A majority of cases of grade ≥4 CRS occurred during CAR T-cell dose finding. Multivariable analysis of baseline characteristics identified high marrow tumor burden, lymphodepletion using cyclophosphamide and fludarabine, higher CAR T-cell dose, thrombocytopenia before lymphodepletion, and manufacturing of CAR T cells without selection of CD8+ central memory T cells as independent predictors of CRS. Severe CRS was characterized by hemodynamic instability, capillary leak, and consumptive coagulopathy. Angiopoietin-2 and von Willebrand factor, which are biomarkers of endothelial activation, were increased during severe CRS and also before lymphodepletion in patients who subsequently developed CRS. We describe a classification-tree algorithm to guide studies of early intervention after CAR T-cell infusion for patients at high risk of severe CRS. These data provide a framework for early intervention studies to facilitate safer application of effective CD19 CAR T-cell therapy.
© 2017 by The American Society of Hematology.
Figures
Comment in
-
CAR emissions: cytokines tell the story.Blood. 2017 Nov 23;130(21):2238-2240. doi: 10.1182/blood-2017-10-808592. Blood. 2017. PMID: 29170192 No abstract available.
References
-
- Turtle CJ, Hanafi LA, Li D, et al. CD19 CAR-T cells are highly effective in ibrutinib-refractory chronic lymphocytic leukemia [abstract]. Blood. 2016;128(22). Abstract 56.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
