

Incidental colorectal focal 18 F-FDG uptake: a novel indication for colonoscopy
- PMID: 28924601
- PMCID: PMC5597934
- DOI: 10.1055/s-0043-116384
Incidental colorectal focal 18 F-FDG uptake: a novel indication for colonoscopy
Abstract
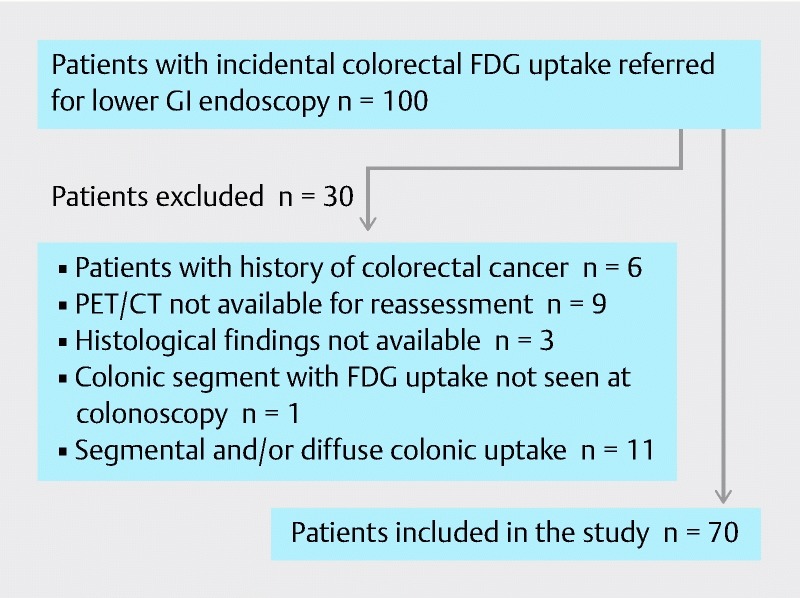
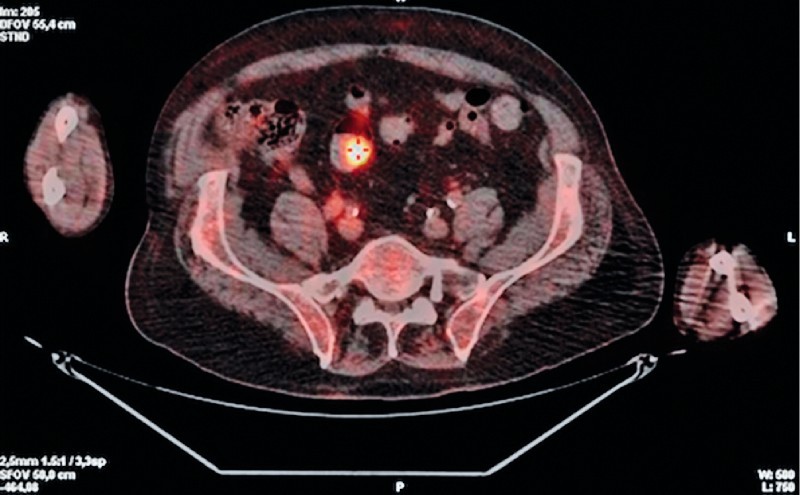
Background and study aims: The relevance of incidental colorectal focal 18 F-FDG PET/CT uptake is debatable. All patients who were referred for colonoscopy because of incidental colonic focal FDG uptake were included in this retrospective study.
Patients and methods: PET/CT imaging characteristics were reviewed by a nuclear physician who was blinded to endoscopic and histopathological findings to determine the location of FDG uptake sites and to measure the maximum standardized uptake values (SUVmax) and metabolic volume (MV). Endoscopic findings were categorized as malignant lesions (ML), high-risk polyps (HRP), low-risk polyps (LRP) or other non-neoplastic lesions (NNL).
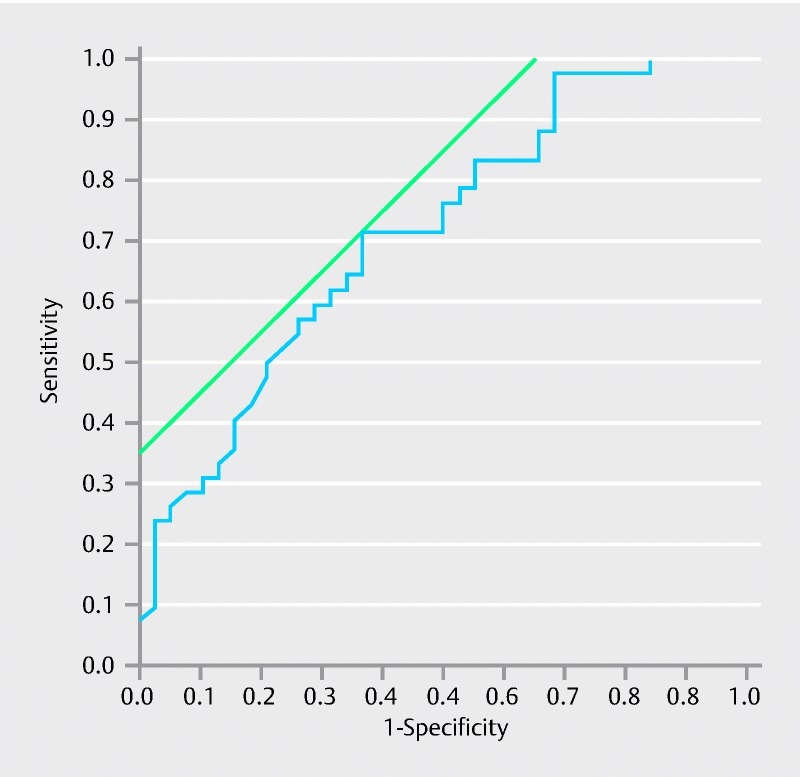
Results: Seventy patients with 84 foci of FDG uptake were included. The proportions of true-positive (lesions found at colonoscopy at the same location) and false-positive (no lesion at colonoscopy) PET/CT findings were 65.5 % (n = 55) and 34.5 % (n = 29). Median SUVmax values did not differ between true-positive and false-positive findings ( P = 0.27). Median MV30 values differed significantly between true-positive (5.5 cm 3 , [3.3 - 10.9 cm 3 ]) and false-positive (9.7 cm 3 , [5.2 - 40.8 cm 3 ]) findings ( P = 0.015). Among the 55 true-positive FDG uptake sites, there were 14 (25.5 %) malignant lesions, 30 (54.5 %) HRP, 4 (7.3 %) LRP, and 7 (12.7 %) NNL. Median MV30 values differed significantly between advanced neoplasia (5.0 cm 3 , [2.9 - 9.7 cm 3 ]) and other endoscopic findings (9.4 cm 3 , [5.2 - 39.8 cm 3 ]) ( P = 0.001); the AUROC was 0.71. By per-colonic segment analysis, the distribution of true-positive, false-negative, false-positive, and true-negative FDG PET/CT findings was as follows: 21.5 %, 14.2 %, 11.5 %, and 52.8 %, respectively.
Conclusion: Our study demonstrates that follow-up complete colonoscopy is mandatory in all patients with incidental colorectal focal 18 F-FDG PET/CT uptake.
Conflict of interest statement
Figures
References
-
- Agress H, Cooper B Z. Detection of clinically unexpected malignant and premalignant tumors with whole-body FDG PET: histopathologic comparison. Radiology. 2004;230:417–422. - PubMed
-
- Even-Sapir E, Lerman H, Gutman M et al. The presentation of malignant tumours and pre-malignant lesions incidentally found on PET-CT. Eur J Nucl Med Mol Imaging. 2006;33:541–552. - PubMed
-
- Ozkol V, Alper E, Aydin N et al. The clinical value of incidental 18F-fluorodeoxyglucose-avid foci detected on positron emission tomography/computed tomography. Nucl Med Commun. 2010;31:128–136. - PubMed
-
- Ishimori T, Patel P V, Wahl R L. Detection of unexpected additional primary malignancies with PET/CT. J Nucl Med. 2005;46:752–757. - PubMed
-
- Beatty J S, Williams H T, Aldridge B A et al. Incidental PET/CT findings in the cancer patient: how should they be managed? Surgery. 2009;146:274–281. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous