

Self-monitoring of blood pressure in hypertension: A systematic review and individual patient data meta-analysis
- PMID: 28926573
- PMCID: PMC5604965
- DOI: 10.1371/journal.pmed.1002389
Self-monitoring of blood pressure in hypertension: A systematic review and individual patient data meta-analysis
Abstract
Background: Self-monitoring of blood pressure (BP) appears to reduce BP in hypertension but important questions remain regarding effective implementation and which groups may benefit most. This individual patient data (IPD) meta-analysis was performed to better understand the effectiveness of BP self-monitoring to lower BP and control hypertension.
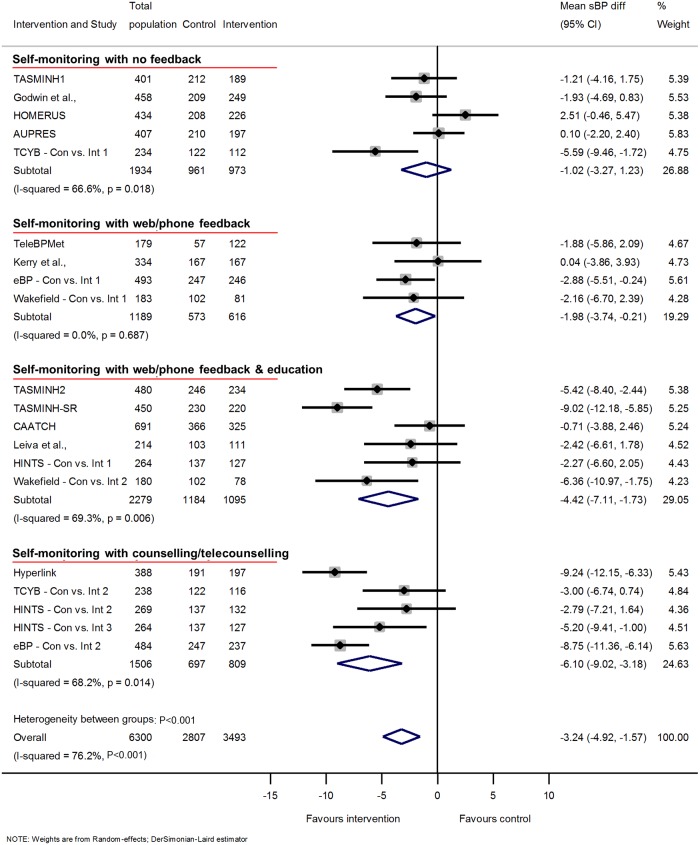
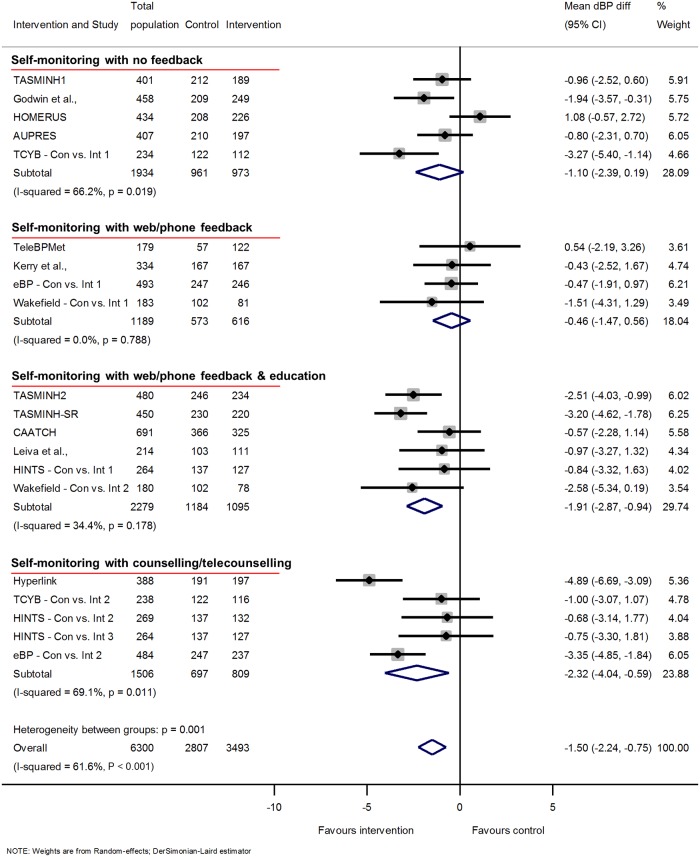
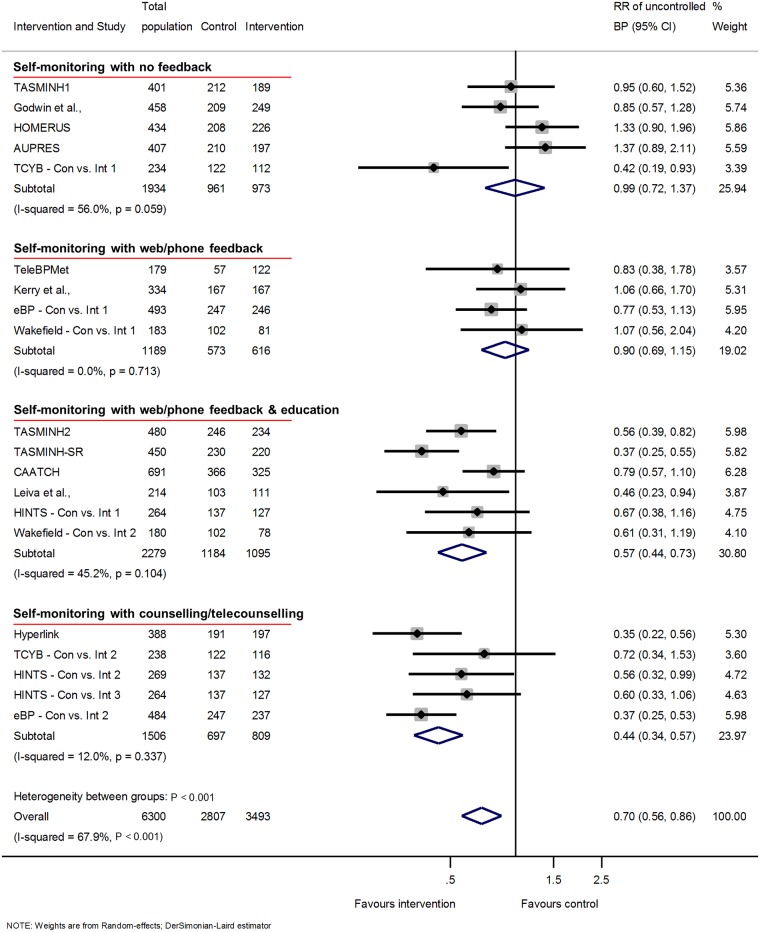
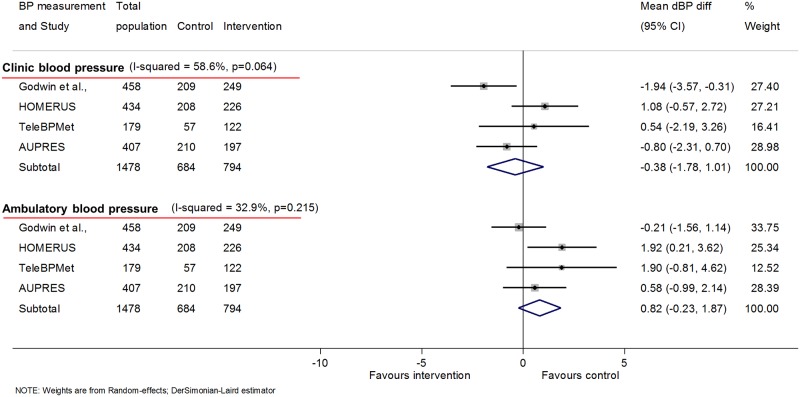
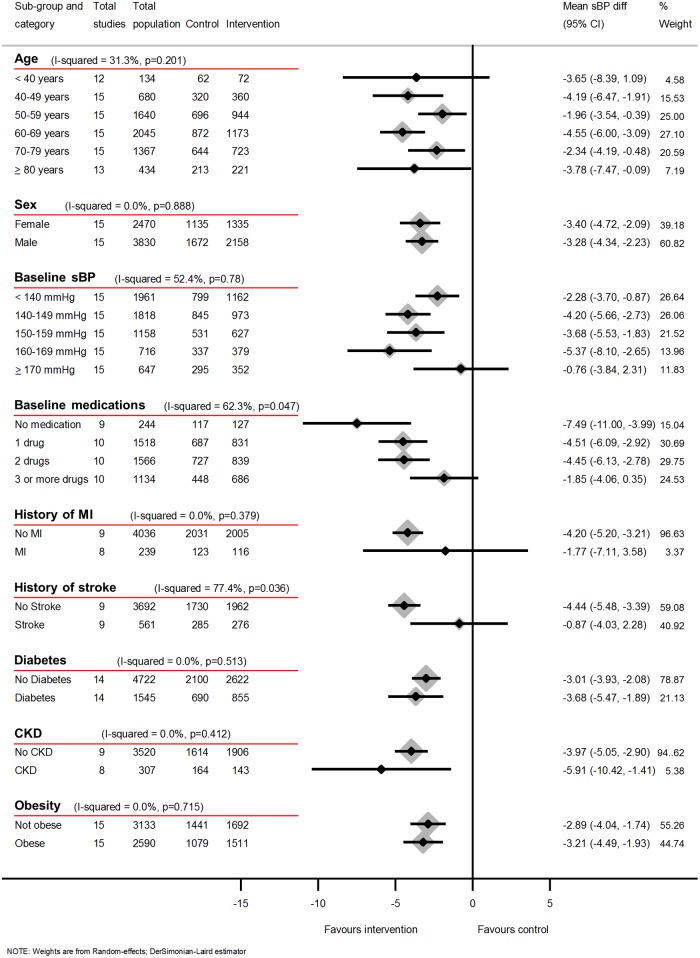
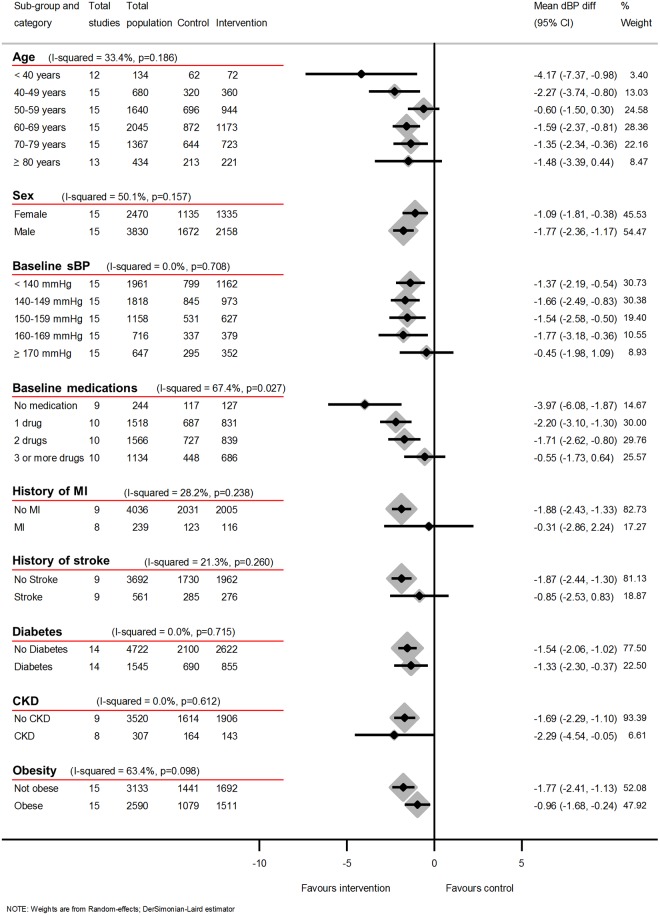
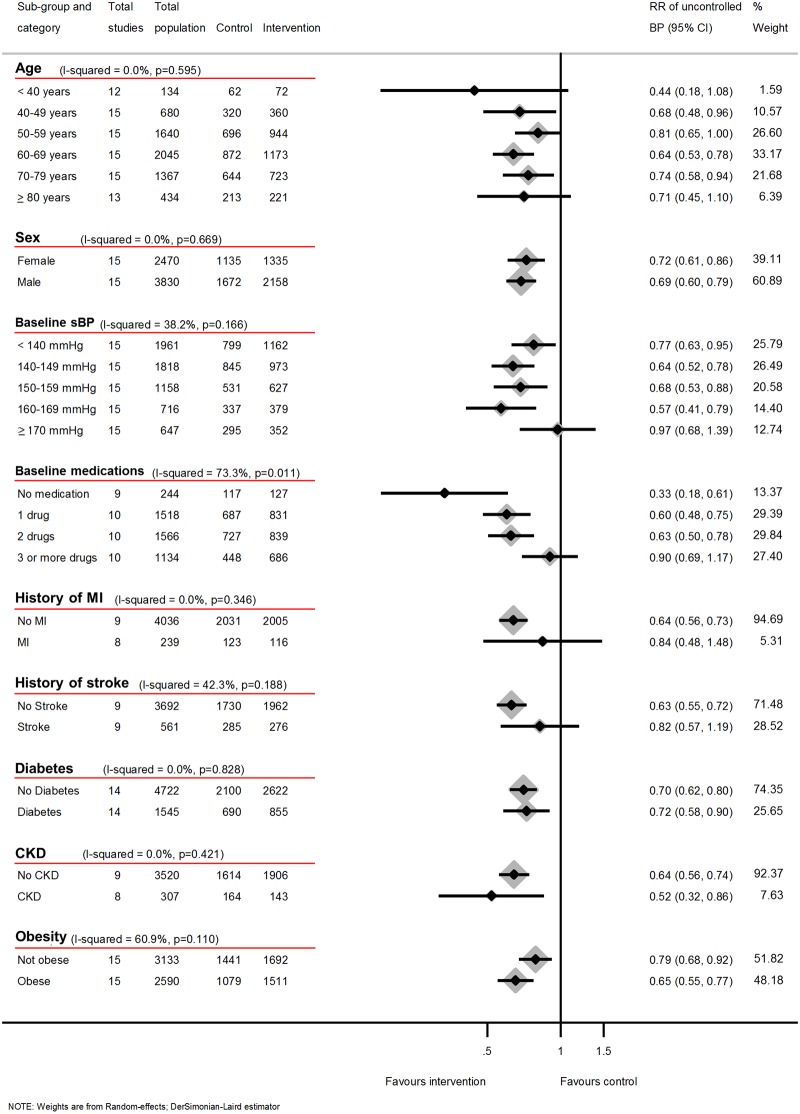
Methods and findings: Medline, Embase, and the Cochrane Library were searched for randomised trials comparing self-monitoring to no self-monitoring in hypertensive patients (June 2016). Two reviewers independently assessed articles for eligibility and the authors of eligible trials were approached requesting IPD. Of 2,846 articles in the initial search, 36 were eligible. IPD were provided from 25 trials, including 1 unpublished study. Data for the primary outcomes-change in mean clinic or ambulatory BP and proportion controlled below target at 12 months-were available from 15/19 possible studies (7,138/8,292 [86%] of randomised participants). Overall, self-monitoring was associated with reduced clinic systolic blood pressure (sBP) compared to usual care at 12 months (-3.2 mmHg, [95% CI -4.9, -1.6 mmHg]). However, this effect was strongly influenced by the intensity of co-intervention ranging from no effect with self-monitoring alone (-1.0 mmHg [-3.3, 1.2]), to a 6.1 mmHg (-9.0, -3.2) reduction when monitoring was combined with intensive support. Self-monitoring was most effective in those with fewer antihypertensive medications and higher baseline sBP up to 170 mmHg. No differences in efficacy were seen by sex or by most comorbidities. Ambulatory BP data at 12 months were available from 4 trials (1,478 patients), which assessed self-monitoring with little or no co-intervention. There was no association between self-monitoring and either lower clinic or ambulatory sBP in this group (clinic -0.2 mmHg [-2.2, 1.8]; ambulatory 1.1 mmHg [-0.3, 2.5]). Results for diastolic blood pressure (dBP) were similar. The main limitation of this work was that significant heterogeneity remained. This was at least in part due to different inclusion criteria, self-monitoring regimes, and target BPs in included studies.
Conclusions: Self-monitoring alone is not associated with lower BP or better control, but in conjunction with co-interventions (including systematic medication titration by doctors, pharmacists, or patients; education; or lifestyle counselling) leads to clinically significant BP reduction which persists for at least 12 months. The implementation of self-monitoring in hypertension should be accompanied by such co-interventions.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: RJM has received research funding in terms of blood pressure monitors from Omron and Lloyds Healthcare; has received expenses and an honorarium from the Japanese Society of Hypertension and American Society of Nephrology. WJV is now employed by Microlife but was not at the time that the data contributed were collected. FDRH has in the past received limited free or subsidised BP measuring devices from Microlife and Omron to support hypertension research where there was no input from the companies to the design, funding, delivery, analysis, or interpretation of that research. SO is a consultant of Biotechmed Ltd. (provider of blood pressure telemonitoring services). SK has received research funding in terms of blood pressure monitors from Omron. HBB has received grant funding to Duke University from Sanofi, Johnson and Johnson, Takeda, WestMeadVaco, and Improved patient Outcome; has received an honorarium from Walgreens, Genentech, Sanofi; and has received funds for consulting for Sanofi. JPS received an MRC Strategic Skills Postdoctoral Fellowship (2013-2016) and now receives funding from the NIHR Oxford Collaborations for Leadership in Applied Health Research and Care. AB owns stocks in Insight Telehealth Systems LLC. MG received a research grant from the Heart and Stroke Foundation of Ontario prior to this work to conduct a study on self-monitoring of blood pressure, data from which are included in this meta-analysis. JG has held unrestricted investigator initiated grants from Pfizer and Boehringer-Ingelheim (BI) for unrelated research; is a member of the Lung Foundation Australia's (LFA) COPD-X guidelines committee. Pfizer, BI, or LFA did not have any role in my decision to participate in the work submitted by Tucker et al. IK has received travel grants and honoraria for speaking or participation at meetings from Sanofi-Genzyme and Shire concerning Fabry disease; has participated in clinical studies concerning diabetic nephropathy and hyperlipidemia sponsored by Bayer, Boehringer-Ingelheim, Merck Sharp and Dome and Pfizer.
Figures

Comment in
-
Review: In hypertension, BP self-monitoring interventions improve BP levels and BP control at 12 months.Ann Intern Med. 2018 Feb 20;168(4):JC16. doi: 10.7326/ACPJC-2018-168-4-016. Ann Intern Med. 2018. PMID: 29459953 No abstract available.
References
-
- Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ. 2009;338: b1665 doi: 10.1136/bmj.b1665 - DOI - PMC - PubMed
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, et al. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335: 827–38. - PubMed
-
- Wolf-Maier K, Cooper RS, Kramer H, Banegas JR, Giampaoli S, Joffres MR, et al. Hypertension treatment and control in five European countries, Canada, and the United States. Hypertension. 2004;43: 10–17. Epub 2003/11/26. doi: 10.1161/01.HYP.0000103630.72812.10 - DOI - PubMed
-
- Uhlig K, Patel K, Ip S, Kitsios GD, Balk EM. Self-measured blood pressure monitoring in the management of hypertension: a systematic review and meta-analysis. Ann Intern Med. 2013;159: 185–94. Epub 2013/08/08. doi: 10.7326/0003-4819-159-3-201308060-00008 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
