

Effects of N-acetylcysteine treatment in acute respiratory distress syndrome: A meta-analysis
- PMID: 28928799
- PMCID: PMC5590037
- DOI: 10.3892/etm.2017.4891
Effects of N-acetylcysteine treatment in acute respiratory distress syndrome: A meta-analysis
Abstract
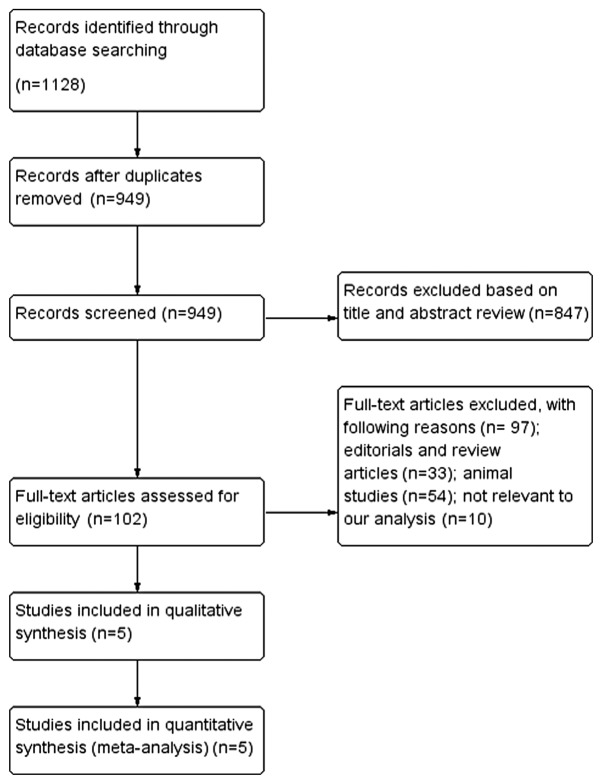
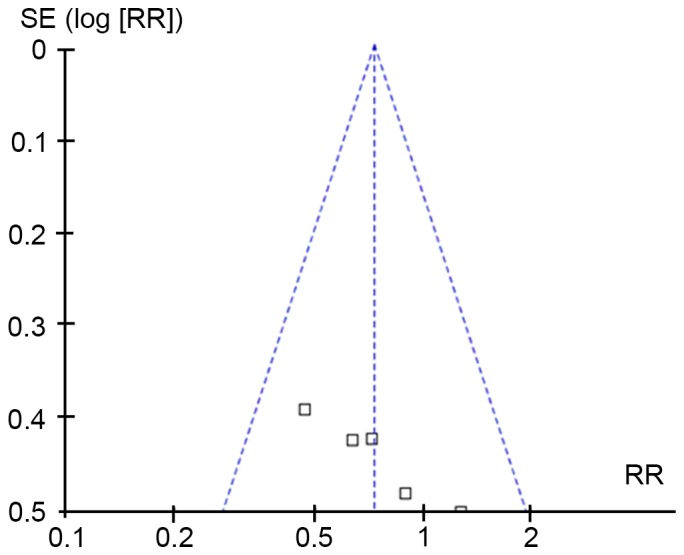
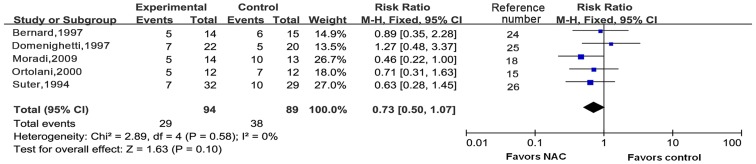
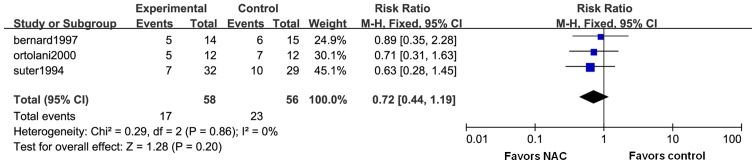
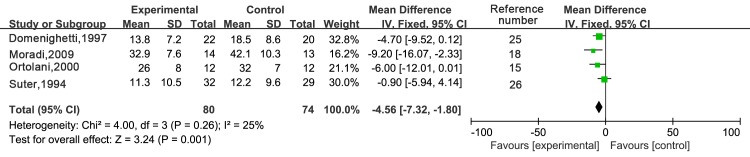
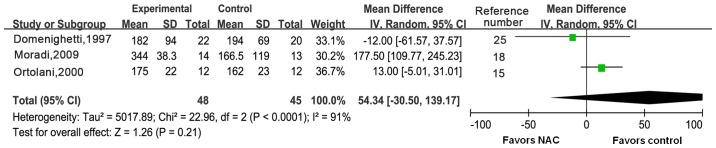
Acute respiratory distress syndrome (ARDS) is a serious complication of acute lung injury. Severe systemic inflammation is the main cause of multiple organ dysfunction and high mortality. Removal of reactive oxygen species by anti-oxidants has been applied in clinical practice. N-acetylcysteine (NAC) is the most commonly used anti-oxidant. However, the benefit of anti-oxidant therapy was not consistently demonstrated by previous studies. In the present study, a meta-analysis was performed to evaluate the effects of NAC for adult patients with ARDS. The PubMed, Cochrane and EMBASE databases were searched to retrieve all of the available randomized controlled trials (RCTs) published until October 2015. Quality evaluation of included studies was performed according to the modified Jadad scale score. The Cochrane Collaboration Review Manager 5.3 software was used to perform the meta-analysis. Five RCTs comprising 183 patients were found to be eligible for inclusion in the meta-analysis. Pooled analysis showed that NAC did not contribute to reduce short-term mortality [risk ratio (RR)=0.73; 95% confidence interval (CI): 0.50-1.07; P=0.10] or 30-day mortality (RR=0.72; 95% CI: 0.44-1.19; P=0.20) when compared with those in the control group. However, duration of intensive care unit (ICU) stay in the NAC group was shortened [weighted mean difference (WMD), -4.56; 95% CI: (-7.32 to -1.80); P=0.001]. There was no significant difference in the ratio of partial arterial oxygen pressure to the fraction of inspired oxygen between the two groups [WMD, 54.34; 95% CI: (-30.50 to 139.17); P=0.21]. No severe adverse reactions were observed in the patients included. Although the duration of ICU stay was shortened, the clinical benefits of NAC were limited for ARDS based on the present meta-analysis. As the number of included trials and patients was small, additional trials are required to provide sufficient evidence for the efficacy of NAC in ARDS.
Keywords: N-acetylcysteine; acute respiratory distress syndrome; mortality; randomized controlled trials; systematic review.
Figures
References
-
- ARDS Definition Task Force, corp-author. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: The Berlin definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Phua J, Badia JR, Adhikari NK, Friedrich JO, Fowler RA, Singh JM, Scales DC, Stather DR, Li A, Jones A, et al. Has mortality from acute respiratory distress syndrome decreased over time?: A systematic review. Am J Respir Crit Care Med. 2009;179:220–227. doi: 10.1164/rccm.200805-722OC. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials