

Imaging Diagnosis of Right Ventricle Involvement in Chagas Cardiomyopathy
- PMID: 28929112
- PMCID: PMC5592008
- DOI: 10.1155/2017/3820191
Imaging Diagnosis of Right Ventricle Involvement in Chagas Cardiomyopathy
Abstract
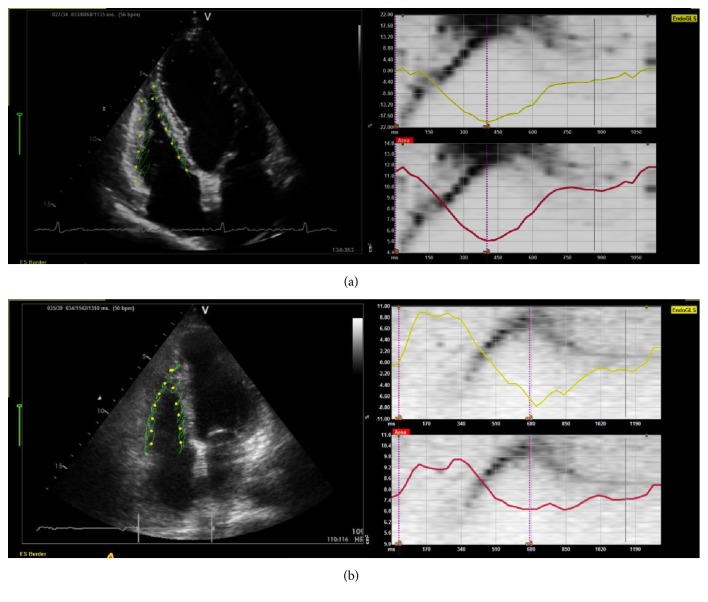
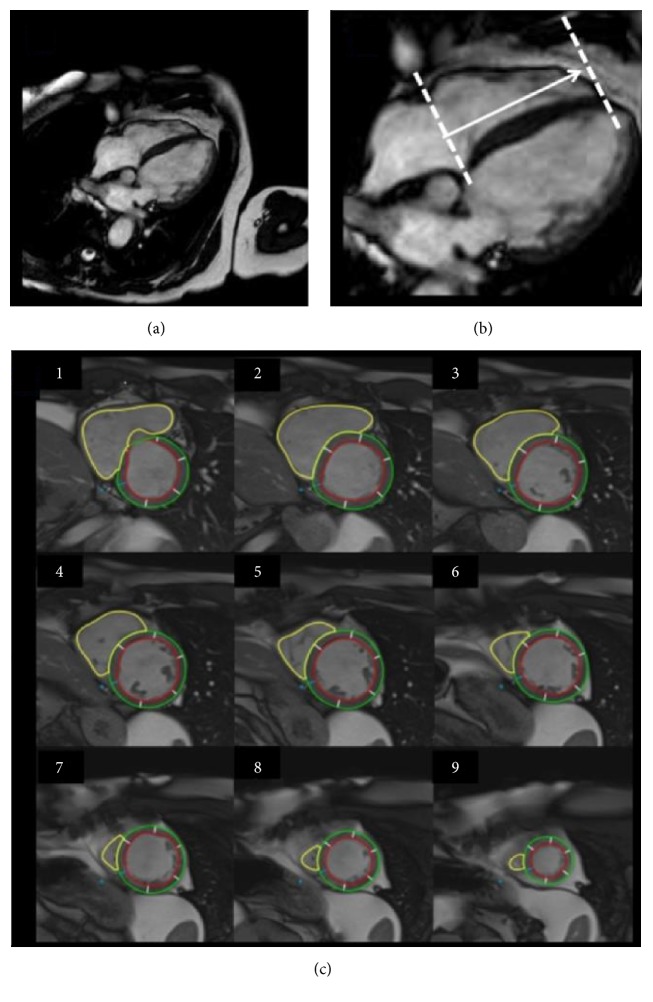
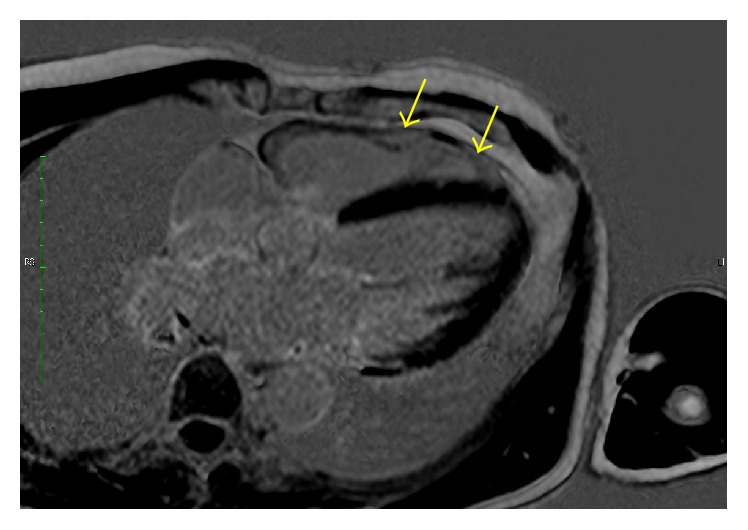
Right ventricle (RV) is considered a neglected chamber in cardiology and knowledge about its role in cardiac function was mostly focused on ventricular interdependence. However, progress on the understanding of myocardium diseases primarily involving the RV led to a better comprehension of its role in health and disease. In Chagas disease (CD), there is direct evidence from both basic and clinical research of profound structural RV abnormalities. However, clinical detection of these abnormalities is hindered by technical limitations of imaging diagnostic tools. Echocardiography has been a widespread and low-cost option for the study of patients with CD but, when applied to the RV assessment, faces difficulties such as the absence of a geometrical shape to represent this cavity. More recently, the technique has evolved to a focused guided RV imaging and myocardial deformation analysis. Also, cardiac magnetic resonance (CMR) has been introduced as a gold standard method to evaluate RV cavity volumes. CMR advantages include precise quantitative analyses of both LV and RV volumes and its ability to perform myocardium tissue characterization to identify areas of scar and edema. Evolution of these cardiac diagnostic techniques opened a new path to explore the pathophysiology of RV dysfunction in CD.
Figures
References
-
- Janicki J. S., Weber K. T. Factors influencing the diastolic pressure-volume relation of the cardiac ventricles. Federation Proceedings. 1980;39(2):133–140. - PubMed
-
- Starr I., Jeffers W. A., Meade R. H., Jr. The absence of conspicuous increments of venous pressure after severe damage to the right ventricle of the dog, with a discussion of the relation between clinical congestive failure and heart disease. American Heart Journal. 1943;26(3):291–301. doi: 10.1016/S0002-8703(43)90325-4. - DOI
-
- Brooks H., Holland R., Al-Sadir J. Right ventricular performance during ischemia: an anatomic and hemodynamic analysis. The American journal of physiology. 1977;233(4):H505–H513. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
