

Weight and Metabolic Outcomes 12 Years after Gastric Bypass
- PMID: 28930514
- PMCID: PMC5737957
- DOI: 10.1056/NEJMoa1700459
Weight and Metabolic Outcomes 12 Years after Gastric Bypass
Abstract
Background: Few long-term or controlled studies of bariatric surgery have been conducted to date. We report the 12-year follow-up results of an observational, prospective study of Roux-en-Y gastric bypass that was conducted in the United States.
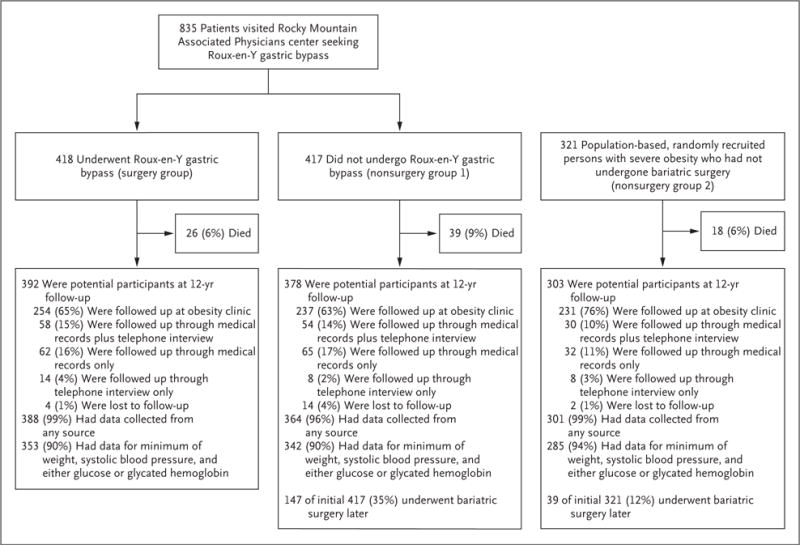
Methods: A total of 1156 patients with severe obesity comprised three groups: 418 patients who sought and underwent Roux-en-Y gastric bypass (surgery group), 417 patients who sought but did not undergo surgery (primarily for insurance reasons) (nonsurgery group 1), and 321 patients who did not seek surgery (nonsurgery group 2). We performed clinical examinations at baseline and at 2 years, 6 years, and 12 years to ascertain the presence of type 2 diabetes, hypertension, and dyslipidemia.
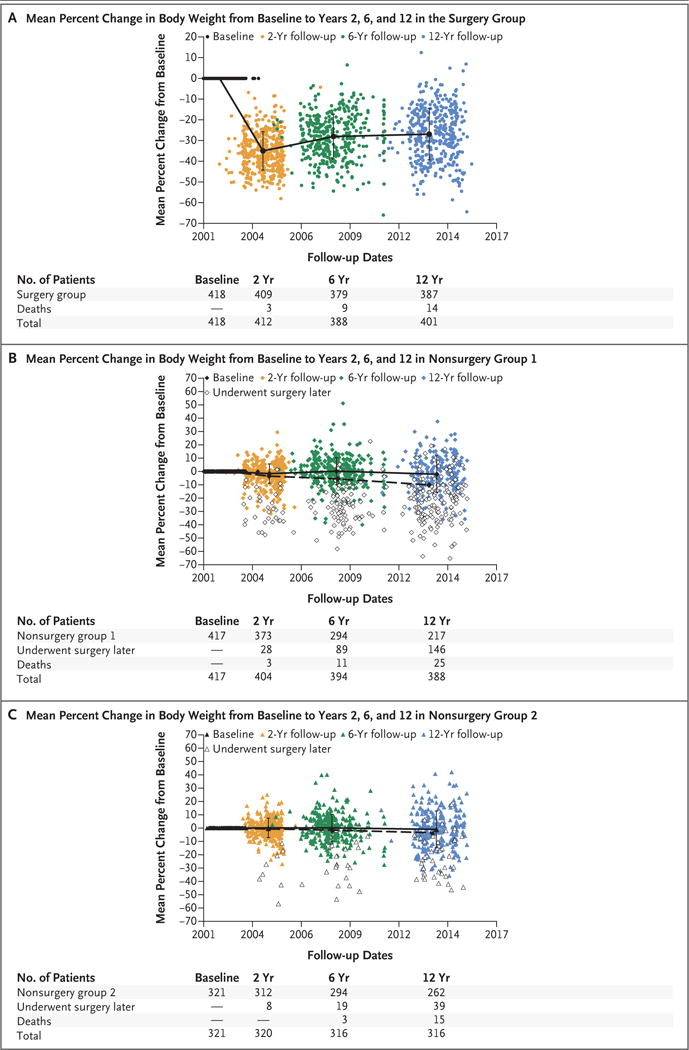
Results: The follow-up rate exceeded 90% at 12 years. The adjusted mean change from baseline in body weight in the surgery group was -45.0 kg (95% confidence interval [CI], -47.2 to -42.9; mean percent change, -35.0) at 2 years, -36.3 kg (95% CI, -39.0 to -33.5; mean percent change, -28.0) at 6 years, and -35.0 kg (95% CI, -38.4 to -31.7; mean percent change, -26.9) at 12 years; the mean change at 12 years in nonsurgery group 1 was -2.9 kg (95% CI, -6.9 to 1.0; mean percent change, -2.0), and the mean change at 12 years in nonsurgery group 2 was 0 kg (95% CI, -3.5 to 3.5; mean percent change, -0.9). Among the patients in the surgery group who had type 2 diabetes at baseline, type 2 diabetes remitted in 66 of 88 patients (75%) at 2 years, in 54 of 87 patients (62%) at 6 years, and in 43 of 84 patients (51%) at 12 years. The odds ratio for the incidence of type 2 diabetes at 12 years was 0.08 (95% CI, 0.03 to 0.24) for the surgery group versus nonsurgery group 1 and 0.09 (95% CI, 0.03 to 0.29) for the surgery group versus nonsurgery group 2 (P<0.001 for both comparisons). The surgery group had higher remission rates and lower incidence rates of hypertension and dyslipidemia than did nonsurgery group 1 (P<0.05 for all comparisons).
Conclusions: This study showed long-term durability of weight loss and effective remission and prevention of type 2 diabetes, hypertension, and dyslipidemia after Roux-en-Y gastric bypass. (Funded by the National Institute of Diabetes and Digestive and Kidney Diseases and others.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Long-term durability of outcomes after bariatric surgery: thinking outside the box.Surg Obes Relat Dis. 2018 Feb;14(2):247. doi: 10.1016/j.soard.2017.10.011. Epub 2017 Oct 26. Surg Obes Relat Dis. 2018. PMID: 29254688 No abstract available.
-
Gastric Bypass Surgery has Long-Term Health Benefits.Am J Nurs. 2018 Jan;118(1):56. doi: 10.1097/01.NAJ.0000529716.93343.6b. Am J Nurs. 2018. PMID: 29280807 No abstract available.
-
Weight and Metabolic Outcomes 12 Years after Gastric Bypass.N Engl J Med. 2018 Jan 4;378(1):93. doi: 10.1056/NEJMc1714001. N Engl J Med. 2018. PMID: 29298158 No abstract available.
-
Weight and Metabolic Outcomes 12 Years after Gastric Bypass.N Engl J Med. 2018 Jan 4;378(1):95. doi: 10.1056/NEJMc1714001. N Engl J Med. 2018. PMID: 29303539 No abstract available.
-
Weight and Metabolic Outcomes 12 Years after Gastric Bypass.N Engl J Med. 2018 Jan 4;378(1):93-4. doi: 10.1056/NEJMc1714001. N Engl J Med. 2018. PMID: 29303540 No abstract available.
-
Überragende Langzeitdaten nach bariatrischer Chirurgie.MMW Fortschr Med. 2018 Jan;160(1):35. doi: 10.1007/s15006-018-0084-1. MMW Fortschr Med. 2018. PMID: 29335950 Review. German. No abstract available.
-
JPEN Journal Club 34. Suspecting Causation in an Association.JPEN J Parenter Enteral Nutr. 2018 May;42(4):826-828. doi: 10.1002/jpen.1155. Epub 2018 Mar 30. JPEN J Parenter Enteral Nutr. 2018. PMID: 29603283 No abstract available.
References
-
- Dixon JB, O’Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299:316–23. - PubMed
-
- Liang Z, Wu Q, Chen B, Yu P, Zhao H, Ouyang X. Effect of laparoscopic Roux-en-Y gastric bypass surgery on type 2 diabetes mellitus with hypertension: a randomized controlled trial. Diabetes Res Clin Pract. 2013;101:50–6. - PubMed
-
- Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet. 2015;386:964–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials