

Variability in Usual Care Mechanical Ventilation for Pediatric Acute Respiratory Distress Syndrome: Time for a Decision Support Protocol?
- PMID: 28930815
- PMCID: PMC5679099
- DOI: 10.1097/PCC.0000000000001319
Variability in Usual Care Mechanical Ventilation for Pediatric Acute Respiratory Distress Syndrome: Time for a Decision Support Protocol?
Abstract
Objectives: Although pediatric intensivists philosophically embrace lung protective ventilation for acute lung injury and acute respiratory distress syndrome, we hypothesized that ventilator management varies. We assessed ventilator management by evaluating changes to ventilator settings in response to blood gases, pulse oximetry, or end-tidal CO2. We also assessed the potential impact that a pediatric mechanical ventilation protocol adapted from National Heart Lung and Blood Institute acute respiratory distress syndrome network protocols could have on reducing variability by comparing actual changes in ventilator settings to those recommended by the protocol.
Design: Prospective observational study.
Setting: Eight tertiary care U.S. PICUs, October 2011 to April 2012.
Patients: One hundred twenty patients (age range 17 d to 18 yr) with acute lung injury/acute respiratory distress syndrome.
Measurements and main results: Two thousand hundred arterial and capillary blood gases, 3,964 oxygen saturation by pulse oximetry, and 2,757 end-tidal CO2 values were associated with 3,983 ventilator settings. Ventilation mode at study onset was pressure control 60%, volume control 19%, pressure-regulated volume control 18%, and high-frequency oscillatory ventilation 3%. Clinicians changed FIO2 by ±5 or ±10% increments every 8 hours. Positive end-expiratory pressure was limited at ~10 cm H2O as oxygenation worsened, lower than would have been recommended by the protocol. In the first 72 hours of mechanical ventilation, maximum tidal volume/kg using predicted versus actual body weight was 10.3 (8.5-12.9) (median [interquartile range]) versus 9.2 mL/kg (7.6-12.0) (p < 0.001). Intensivists made changes similar to protocol recommendations 29% of the time, opposite to the protocol's recommendation 12% of the time and no changes 56% of the time.
Conclusions: Ventilator management varies substantially in children with acute respiratory distress syndrome. Opportunities exist to minimize variability and potentially injurious ventilator settings by using a pediatric mechanical ventilation protocol offering adequately explicit instructions for given clinical situations. An accepted protocol could also reduce confounding by mechanical ventilation management in a clinical trial.
Figures
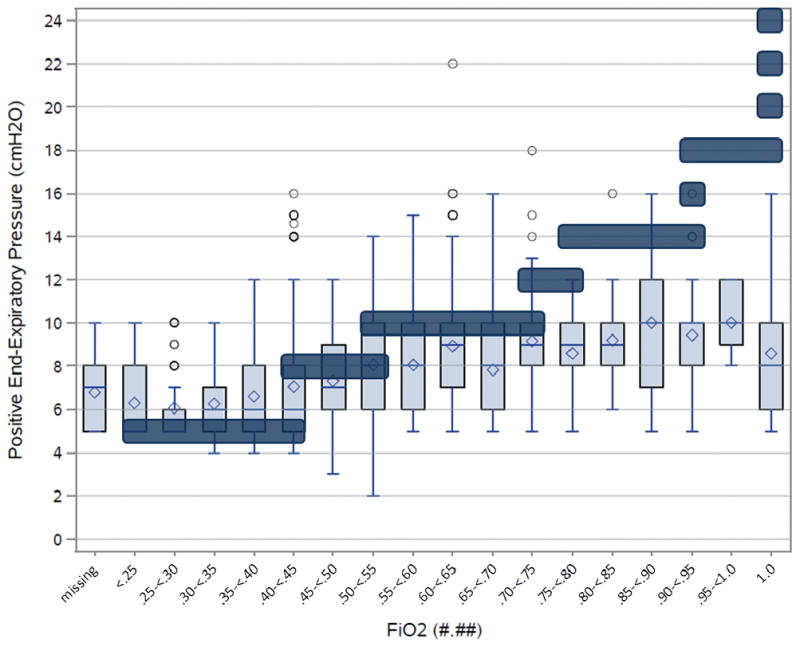
Actual CPCCRN data (Light blue boxes); Mean value (◇), Median (Bar), IQR (Box), Range (Whiskers), Outliers (○), Protocol Targets (Dark blue bars).
Missing values are for 15 of the 3504 PEEP/FiO2 observations for which no FiO2 was recorded. In addition, there were 26 observations excluded where no PEEP was recorded.
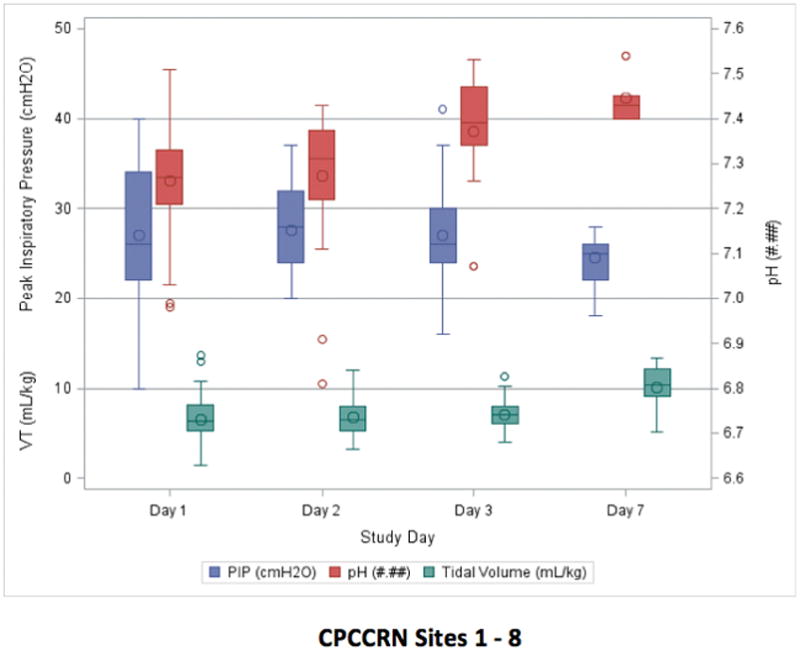
Tidal volumes were maintained in the 7–8 ml/kg range for this group of patients with severe pediatric ARDS over the first three days. The resolution of disease over the week is implied by decreasing peak pressures and rising pHs with tidal volumes having increased up to approximately 11 ml/kg ABW.
Mean value (◇), Median (Bar), IQR (Box), Range (Whiskers), Outliers (○).
Comment in
-
The Quest for the Holy Grail of Optimizing Mechanical Ventilation and Protecting the Lung in Mechanically Ventilated Infants and Children.Pediatr Crit Care Med. 2017 Nov;18(11):1075-1076. doi: 10.1097/PCC.0000000000001324. Pediatr Crit Care Med. 2017. PMID: 29099451 No abstract available.
Similar articles
-
Poor Adherence to Lung-Protective Mechanical Ventilation in Pediatric Acute Respiratory Distress Syndrome.Pediatr Crit Care Med. 2016 Oct;17(10):917-923. doi: 10.1097/PCC.0000000000000903. Pediatr Crit Care Med. 2016. PMID: 27513687 Free PMC article.
-
Adherence to Lung-Protective Ventilation Principles in Pediatric Acute Respiratory Distress Syndrome: A Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology Study.Crit Care Med. 2021 Oct 1;49(10):1779-1789. doi: 10.1097/CCM.0000000000005060. Crit Care Med. 2021. PMID: 34259438 Free PMC article.
-
Variability in usual care mechanical ventilation for pediatric acute lung injury: the potential benefit of a lung protective computer protocol.Intensive Care Med. 2011 Nov;37(11):1840-8. doi: 10.1007/s00134-011-2367-1. Epub 2011 Oct 1. Intensive Care Med. 2011. PMID: 21965099 Free PMC article.
-
Ventilatory support in children with pediatric acute respiratory distress syndrome: proceedings from the Pediatric Acute Lung Injury Consensus Conference.Pediatr Crit Care Med. 2015 Jun;16(5 Suppl 1):S51-60. doi: 10.1097/PCC.0000000000000433. Pediatr Crit Care Med. 2015. PMID: 26035364
-
Implementation of a low tidal volume ventilation protocol for patients with acute lung injury or acute respiratory distress syndrome.Respir Care. 2001 Oct;46(10):1024-37. Respir Care. 2001. PMID: 11572755 Review.
Cited by
-
Nonadherence to appropriate tidal volume and PEEP in children with pARDS at a single center.Pediatr Pulmonol. 2022 Oct;57(10):2464-2473. doi: 10.1002/ppul.26060. Epub 2022 Jul 14. Pediatr Pulmonol. 2022. PMID: 35778788 Free PMC article.
-
Positive End-Expiratory Pressure Lower Than the ARDS Network Protocol Is Associated with Higher Pediatric Acute Respiratory Distress Syndrome Mortality.Am J Respir Crit Care Med. 2018 Jul 1;198(1):77-89. doi: 10.1164/rccm.201707-1404OC. Am J Respir Crit Care Med. 2018. PMID: 29373802 Free PMC article.
-
The longitudinal course of pediatric acute respiratory distress syndrome and its time to resolution: A prospective observational study.Front Pediatr. 2022 Nov 22;10:993175. doi: 10.3389/fped.2022.993175. eCollection 2022. Front Pediatr. 2022. PMID: 36483473 Free PMC article.
-
Mechanical power in pediatric acute respiratory distress syndrome: a PARDIE study.Crit Care. 2022 Jan 3;26(1):2. doi: 10.1186/s13054-021-03853-6. Crit Care. 2022. PMID: 34980228 Free PMC article.
-
Reply to Tremlett and Kanthimathinathan and to Koopman and Kneyber.Am J Respir Crit Care Med. 2018 Sep 15;198(6):823-824. doi: 10.1164/rccm.201806-1039LE. Am J Respir Crit Care Med. 2018. PMID: 29958000 Free PMC article. No abstract available.
References
-
- Santschi M, Jouvet P, Leclerc F, et al. Acute lung injury in children: Therapeutic practice and feasibility of international clinical trials. Pediatr Crit Care Med. 2010;11(6):681–9. - PubMed
-
- ARDSNet. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342(18):1301–8. - PubMed
-
- Putensen C, Theuerkauf N, Zinserling J, et al. Meta-analysis: ventilation strategies and outcomes of the acute respiratory distress syndrome and acute lung injury. Ann Intern Med. 2009;151(8):566–76. - PubMed
-
- Villar J, Kacmarek RM, Perez-Mendez L, et al. A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome in persistent acute respiratory distress syndrome: a randomized, controlled trial. Crit Care Med. 2006;34(5):1311–8. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD063108/HD/NICHD NIH HHS/United States
- R21 HD061870/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
