

Cronkhite-Canada syndrome associated with colon cancer metastatic to liver: A case report
- PMID: 28930817
- PMCID: PMC5617684
- DOI: 10.1097/MD.0000000000007466
Cronkhite-Canada syndrome associated with colon cancer metastatic to liver: A case report
Abstract
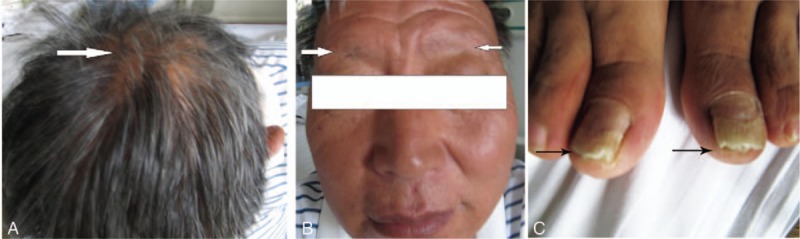
Rationale: Cronkhite-Canada Syndrome (CCS) is an idiopathic, nonhereditary syndrome haracterized by gastrointestinal (GI) polyposis and ectodermal changes including alopecia, onychatrophia, and pigmentation. CCS colon polyps were previously considered to be benign neoplasms. However, serrated adenoma was reported to be associated with malignant neoplasms in some cases of gastric and colorectal carcinomas, and esophageal cancers. Although malignant colon and gastric cancer have been reported in CCS, reports of distant metastasis have been rare in CCS.
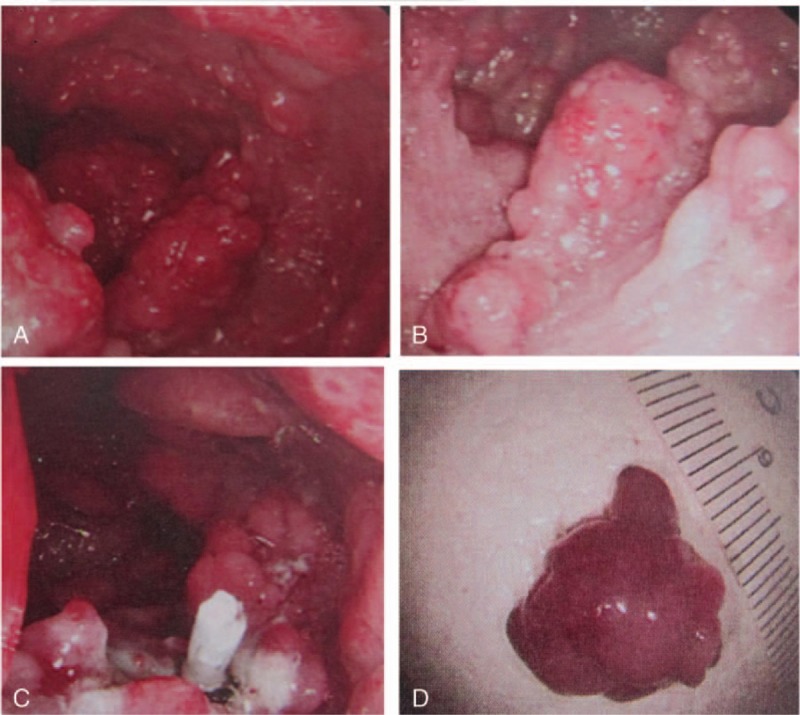
Patient concerns: A 58-year-old male was referred from a nearby hospital with diarrhea and weight loss. The patient was hypoproteinemia (17.9 g/L), and multiple polyps were observed in the large intestine. He also had alopecia, onychatrophia, and dysgeusia.
Diagnoses: The presence of multiple polyps and associated symptoms of alopecia, onychatrophia, pigmentation, and dysgeusia informed the diagnosis of CCS.
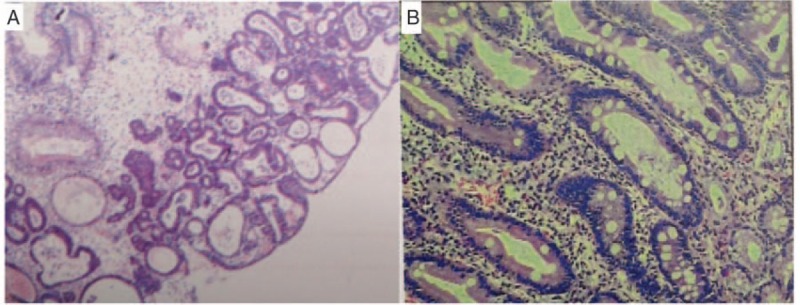
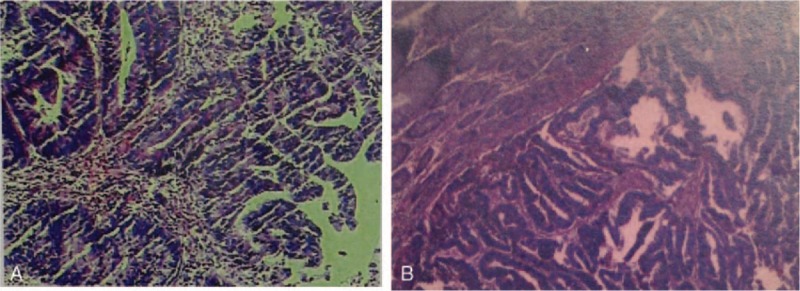
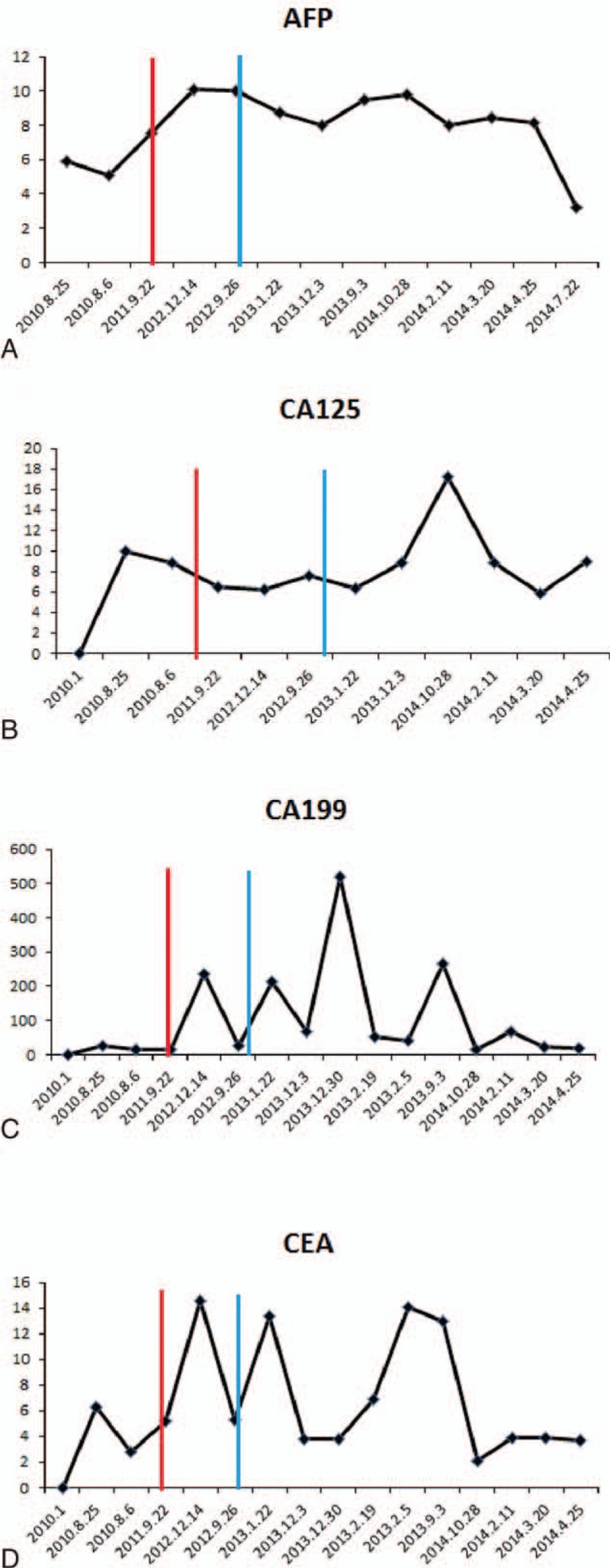
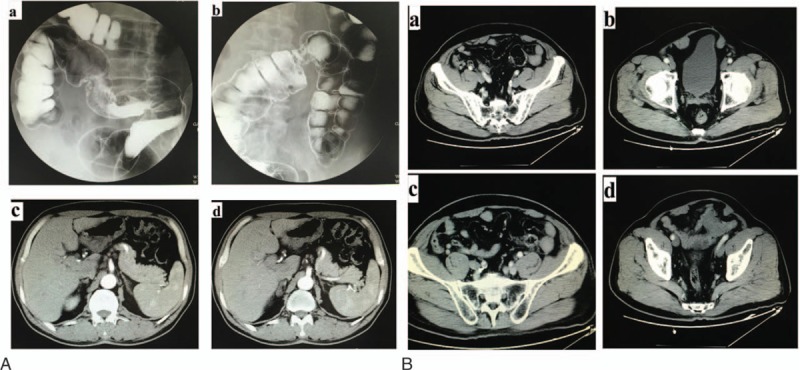
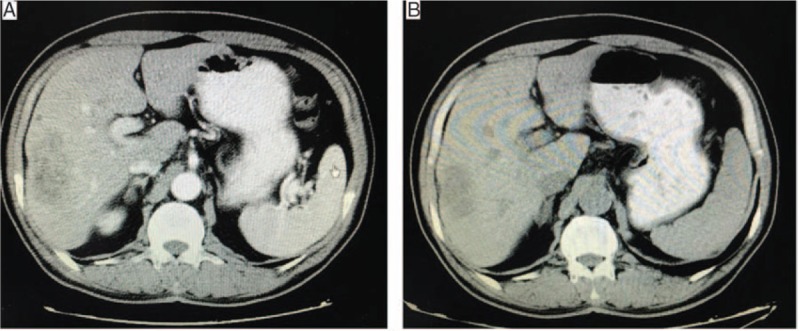
Interventions: He was treated with 20mg dexamethasone acetate per day for about 3 months, 10 mg for about 9 month, 5 mg for about 1 year, and then maintained on 5 mg daily. Three years after starting treatment, colonoscopy revealed colon cancer and colon adenomas. A sigmoidectomy revealed 4 well-differentiated adenocarcinomas of the ulcerating type in the sigmoid colon, and tubularadenomas throughout the rest of the large intestine. He was treated with FOLFOX6 for 6 months. At this stage liver metastasis was found. A right hepatectomy was performed confirming hepatic metastasis of colonic adenocarcinoma, which was GPC-3(-), CD34(-), CK20(+), CDX-2(+), Hep(-), CK19(+), and CK8(+).The patient received 3 courses of hepatic arterial infusion chemotherapy.
Outcomes: The patient's status has been stable for more than 2 years, and there was no tumor recurrence or metastasis occurred.
Lessons: CCS is a rare cause of multiple polyposis most often treated with hormone therapy. Regular follow-ups are very important to ensure discovery of malignant tumors at an early stage. Studies with longer-term observations and larger sample sizes will be required to confirm these observations. However, characterization of molecular markers for the early detection of malignant transformation that might allow less invasive and more cost-effective surveillance of colon cancer is urgently sought.
Conflict of interest statement
This study was supported by the Beijing Municipal Administration of Hospitals’ Youth Program (code: QML20150107) (to Jing Wang), Rising Star Program from Beijing Friendship Hospital, Capital Medical University (yyqdkt2014–10) (to Jing Wang), the Capital Health Research and Development of special (2016–4–1112) (to Jing Wang), and the traditional Chinese Medicine Science and Technology Development Fund project of Beijing (QN2015–10). The authors declare no conflicts of interest.
Figures
Similar articles
-
Cronkhite-Canada syndrome complicated with multiple gastric cancers and multiple colon adenomas.Am J Case Rep. 2013 Apr 26;14:120-8. doi: 10.12659/AJCR.889083. Print 2013. Am J Case Rep. 2013. PMID: 23826450 Free PMC article.
-
[A case of Cronkhite-Canada syndrome with multiple colon adenomas and early colon cancers].Nihon Shokakibyo Gakkai Zasshi. 2011 May;108(5):778-86. Nihon Shokakibyo Gakkai Zasshi. 2011. PMID: 21558745 Japanese.
-
Case report of patient with a Cronkhite-Canada syndrome: sustained remission after treatment with corticosteroids and mesalazine.BMC Gastroenterol. 2019 Feb 27;19(1):36. doi: 10.1186/s12876-019-0944-x. BMC Gastroenterol. 2019. PMID: 30813906 Free PMC article.
-
Cronkhite-Canada syndrome: A case report and literature review.Medicine (Baltimore). 2024 Oct 25;103(43):e40242. doi: 10.1097/MD.0000000000040242. Medicine (Baltimore). 2024. PMID: 39470508 Free PMC article. Review.
-
Cronkhite-Canada syndrome associated with esophageal and gastric cancers: report of a case.Surg Today. 2015 Jun;45(6):777-82. doi: 10.1007/s00595-014-0977-2. Epub 2014 Jul 10. Surg Today. 2015. PMID: 25008327 Review.
Cited by
-
Cronkhite-Canada Syndrome Associated With Superficial Esophageal Carcinoma: A Case Report and Literature Review.Front Med (Lausanne). 2022 Mar 25;9:855336. doi: 10.3389/fmed.2022.855336. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35402458 Free PMC article.
-
Cronkhite-Canada syndrome: A case report.Oncol Lett. 2018 Jun;15(6):8447-8453. doi: 10.3892/ol.2018.8409. Epub 2018 Apr 2. Oncol Lett. 2018. PMID: 29805581 Free PMC article.
-
Cronkhite-Canada Syndrome: A Case Report.JNMA J Nepal Med Assoc. 2022 May 5;60(249):473-477. doi: 10.31729/jnma.7407. JNMA J Nepal Med Assoc. 2022. PMID: 35633239 Free PMC article.
References
-
- Cronkhite LW, Jr, Canada WJ. Generalized gastrointestinal polyposis; an unusual syndrome of polyposis, pigmentation, alopecia and onychotrophia. N Engl J Med 1955;252:1011–5. - PubMed
-
- Mason C, Quinlan C, O’Donovan M, et al. Cronkhite Canada syndrome with early colorectal carcinoma in a patient. Ir Med J 2012;105:308–9. - PubMed
-
- Ito M, Matsumoto S, Takayama T, et al. Cronkhite-Canada syndrome associated with esophageal and gastric cancers: report of a case. Surg Today 2015;45:777–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
