

Enhanced recovery program versus traditional care after hepatectomy: A meta-analysis
- PMID: 28930840
- PMCID: PMC5617707
- DOI: 10.1097/MD.0000000000008052
Enhanced recovery program versus traditional care after hepatectomy: A meta-analysis
Abstract
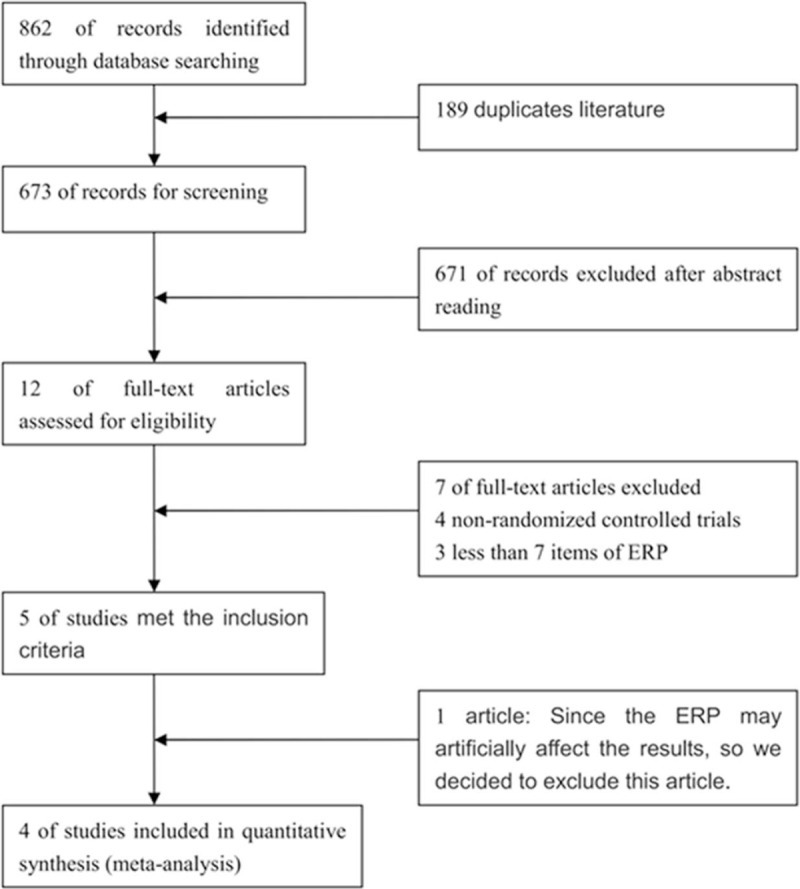
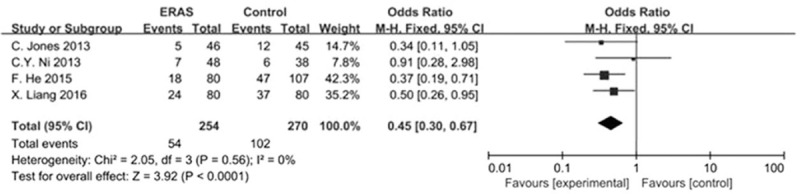
To assess the safety and efficacy of enhanced recovery after surgery (ERAS) as compared with the traditional care in patients undergoing liver surgery and optimization of enhanced recovery programs.Literature, until August 2016, was searched to identify the comparative studies evaluating preoperative hospital stay time, complications, and C-reactive protein (CRP). Pooled odds ratios (OR) or weighted mean differences (WMDs) were calculated with either the fixed or random effect model.These studies included a total of 524 patients: 254 treated with ERAS and 270 with traditional care. The postoperative recovery time and length of hospital stay were significantly better than the control group (WMD -2.72; 95% confidence interval [CI] -3.86 to -1.57; WMD -2.67; 95% CI -3.68 to -1.65, respectively). The overall complications, grade I, and Grand II-V complications were significantly favorable to the ERAS group (OR, 0.45 [95% CI, 0.30-0.67]; OR, 0.55 [95% CI, 0.31-0.98]; OR, 0.49 [95% CI, 0.32-0.76], respectively). The concentration of CRP in the control group was significantly higher than that in the ERAS group on postoperative day 5 (WMD -21.68; 95% CI -29.30 to -14.05). Time to first flatus (WMD -0.93; 95% CI -1.41 to -0.46) was significantly shortened in the ERAS group.The evidence indicates that ERAS following liver surgery is safe, effective, and feasible. Therefore, further are essential for optimizing the ERAS protocols.
Conflict of interest statement
Conflicts of Interest: All authors declare that they have no conflict of interests.
Figures
Similar articles
-
Enhanced recovery after surgery programs in patients undergoing hepatectomy: A meta-analysis.World J Gastroenterol. 2015 Aug 14;21(30):9209-16. doi: 10.3748/wjg.v21.i30.9209. World J Gastroenterol. 2015. PMID: 26290648 Free PMC article. Review.
-
Enhanced recovery after surgery programs versus traditional perioperative care in laparoscopic hepatectomy: A meta-analysis.Int J Surg. 2016 Dec;36(Pt A):274-282. doi: 10.1016/j.ijsu.2016.11.017. Epub 2016 Nov 10. Int J Surg. 2016. PMID: 27840308
-
The efficacy and safety of enhanced recovery after surgery (ERAS) program in laparoscopic digestive system surgery: A meta-analysis of randomized controlled trials.Int J Surg. 2019 Sep;69:108-115. doi: 10.1016/j.ijsu.2019.07.034. Epub 2019 Jul 31. Int J Surg. 2019. PMID: 31376511 Review.
-
Does Postoperative Rehabilitation for Radical Cystectomy Call for Enhanced Recovery after Surgery? A Systematic Review and Meta-analysis.Curr Med Sci. 2019 Feb;39(1):99-110. doi: 10.1007/s11596-019-2006-6. Epub 2019 Mar 13. Curr Med Sci. 2019. PMID: 30868498
-
Enhanced recovery care versus traditional care after laparoscopic liver resections: a randomized controlled trial.Surg Endosc. 2018 Jun;32(6):2746-2757. doi: 10.1007/s00464-017-5973-3. Epub 2017 Dec 12. Surg Endosc. 2018. PMID: 29234943 Clinical Trial.
Cited by
-
Impact of ERAS compliance on the delay between surgery and adjuvant chemotherapy in hepatobiliary and pancreatic malignancies.Langenbecks Arch Surg. 2020 Nov;405(7):959-966. doi: 10.1007/s00423-020-01981-1. Epub 2020 Sep 11. Langenbecks Arch Surg. 2020. PMID: 32918147 Free PMC article.
-
Meta-analysis of Enhanced Recovery After Surgery (ERAS) Protocols in Emergency Abdominal Surgery.World J Surg. 2020 May;44(5):1336-1348. doi: 10.1007/s00268-019-05357-5. World J Surg. 2020. PMID: 31897698
-
Big size is not all, even better!Hepatobiliary Surg Nutr. 2019 Oct;8(5):539-540. doi: 10.21037/hbsn.2019.04.08. Hepatobiliary Surg Nutr. 2019. PMID: 31673551 Free PMC article. No abstract available.
-
Effect of fast-track surgery on postoperative wound pain in patients with prostate cancer: A meta-analysis.Int Wound J. 2023 Sep 22;21(2):e14417. doi: 10.1111/iwj.14417. Online ahead of print. Int Wound J. 2023. Retraction in: Int Wound J. 2025 Mar;22(3):e70354. doi: 10.1111/iwj.70354. PMID: 37737032 Free PMC article. Retracted.
-
Enhanced recovery after surgery society's recommendations for liver surgery reduces non surgical complications.Sci Rep. 2025 Jan 29;15(1):3693. doi: 10.1038/s41598-025-86808-z. Sci Rep. 2025. PMID: 39880966 Free PMC article.
References
-
- Lau WY. Management of hepatocellular carcinoma. J Royal Coll Surg Edinburgh 2002;47:389–99. - PubMed
-
- Palavecino M, Kishi Y, Chun YS, et al. Two-surgeon technique of parenchymal transection contributes to reduced transfusion rate in patients undergoing major hepatectomy: analysis of 1,557 consecutive liver resections. Surgery 2010;147:40–8. - PubMed
-
- Virani S, Michaelson JS, Hutter MM, et al. Morbidity and mortality after liver resection: results of the patient safety in surgery study. J Am Coll Surg 2007;204:1284–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
