

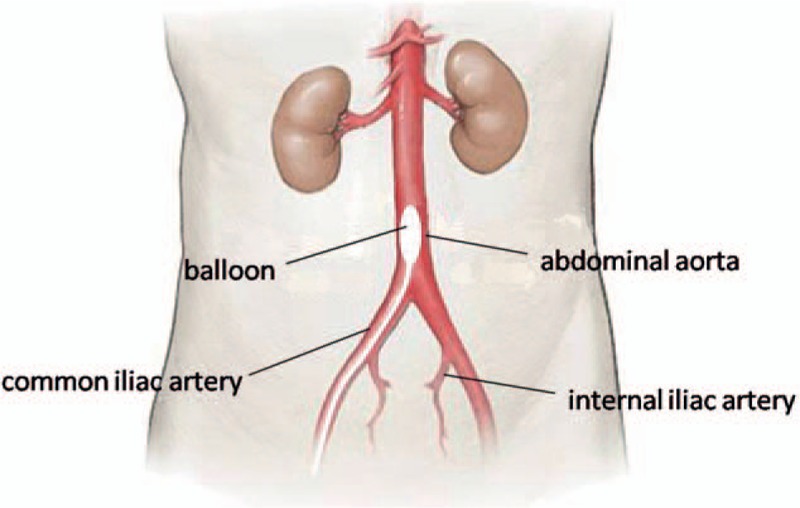
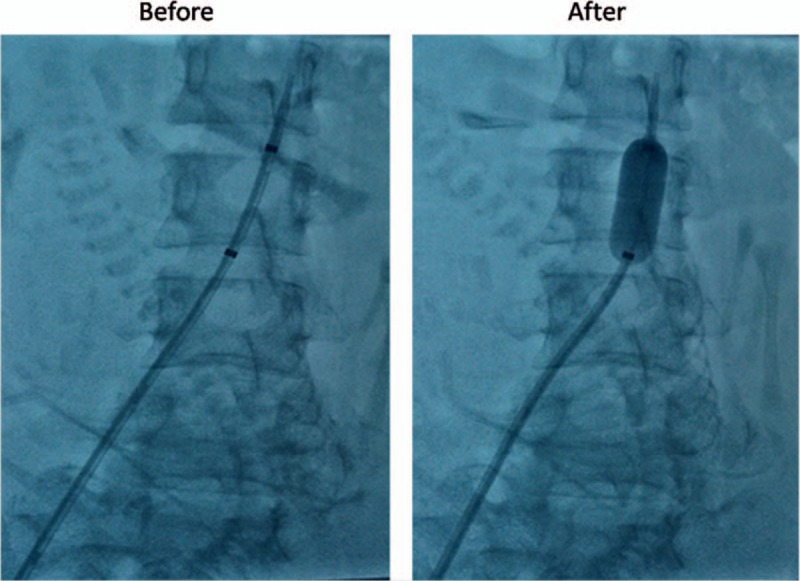
Preoperative infrarenal abdominal aorta balloon catheter occlusion combined with Bakri tamponade reduced maternal morbidity of placenta increta/percreta
- PMID: 28930860
- PMCID: PMC5617727
- DOI: 10.1097/MD.0000000000008114
Preoperative infrarenal abdominal aorta balloon catheter occlusion combined with Bakri tamponade reduced maternal morbidity of placenta increta/percreta
Abstract
Background: Placenta increta/percreta is an increasingly common and life-threatening obstetric complication. It poses a management challenge to clinicians. The present study aimed to evaluate efficacy and safety of preoperative placement of infrarenal abdominal aorta balloon catheter (IAABC) alone or combined with Bakri tamponade for the management of cases with placenta increta/percreta.
Methods: We retrospectively analyzed all cases with placenta increta/percreta at a tertiary referral teaching hospital in China between the year 2014 and 2017. Statistical analysis considered the individual subgroups: IAABC placed group and control group (without IAABC), and compared their maternal-fetal outcomes.
Results: The study covered 86 cases with placenta increta. For cases in the IAABC placed group (n = 48), significant reductions were noted in maternal morbidity including estimated blood loss (EBL), EBL ≥ 2000 mL, blood products transfusions, postpartum hemorrhage, operative time, intensive care unit admission, and postoperative days (P < .05 for all). The overall rate of hysterectomy was much lower (4.2%vs 23.7%, P = .018), compared with those in the control group (n = 38). Furthermore, in the IAABC placed group, hysterectomy was avoided in a further 17 cases combined with Bakri tamponade. In the control group, 10 cases were successful in preserving uterus by Bakri tamponade. Four cases failed and needed reoperation (3 uterine arterial embolism, 1 hysterectomy). There were no differences in fetal outcomes between the 2 groups. Eighteen cases were diagnosed with placenta percreta. Almost all the cases (17/18) inevitably underwent caesarean hysterectomy. Only 1 case was treated with a combination of IAABC and Bakri tamponade, and successfully reserved uterus. No differences were observed in any other outcomes, except for a significant less mean operative time (P = .017) in cases with IAABC placed (n = 10), compared with those without IAABC (n = 8). Only 1 case had a femoral artery thrombosis directly related to IAABC placement and recovered after conservative treatment. There was no maternal or neonatal death in this study.
Conclusion: Prophylactic insertion of IAABC alone or combined with Bakri tamponade should be safe and effective in controlling intraoperative bleeding due to placenta increta, thus hysterectomy could be avoided. It seems to be less beneficial to women with placenta percreta. Bakri tamponade can be a good choice in the management of placenta increta/percreta before more aggressive surgeries.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Comparison of results of Bakri balloon tamponade and caesarean hysterectomy in management of placenta accreta and increta: a retrospective study.J Obstet Gynaecol. 2018 Feb;38(2):194-199. doi: 10.1080/01443615.2017.1340440. Epub 2017 Sep 14. J Obstet Gynaecol. 2018. PMID: 28903630
-
Prophylactic use of intravascular balloon catheters in women with placenta accreta, increta and percreta.Eur J Obstet Gynecol Reprod Biol. 2014 Aug;179:36-41. doi: 10.1016/j.ejogrb.2014.05.007. Epub 2014 May 21. Eur J Obstet Gynecol Reprod Biol. 2014. PMID: 24965977
-
Preoperative Prophylactic Balloon-Assisted Occlusion of the Internal Iliac Arteries in the Management of Placenta Increta/Percreta.Medicina (Kaunas). 2020 Jul 23;56(8):368. doi: 10.3390/medicina56080368. Medicina (Kaunas). 2020. PMID: 32717928 Free PMC article.
-
Clinical evaluation of the effect for prophylactic balloon occlusion in pregnancies complicated with placenta accreta spectrum disorder: A systematic review and meta-analysis.Int J Gynaecol Obstet. 2024 Oct;167(1):109-127. doi: 10.1002/ijgo.15704. Epub 2024 Jun 20. Int J Gynaecol Obstet. 2024. PMID: 38899567
-
Clinical evaluation of prophylactic abdominal aortic balloon occlusion in patients with placenta accreta: a systematic review and meta-analysis.BMC Pregnancy Childbirth. 2019 Jan 15;19(1):30. doi: 10.1186/s12884-019-2175-0. BMC Pregnancy Childbirth. 2019. PMID: 30646863 Free PMC article.
Cited by
-
The effect prophylactic internal iliac artery balloon occlusion in patients with placenta previa or placental accreta spectrum: a systematic review and meta-analysis.Reprod Biol Endocrinol. 2021 Mar 4;19(1):40. doi: 10.1186/s12958-021-00722-3. Reprod Biol Endocrinol. 2021. PMID: 33663536 Free PMC article.
-
Prophylactic occlusion balloon in placenta abnormalities: What every interventional radiologist needs to know.World J Radiol. 2025 Jul 28;17(7):107737. doi: 10.4329/wjr.v17.i7.107737. World J Radiol. 2025. PMID: 40746523 Free PMC article. Review.
-
Successful resuscitation of a patient with pernicious placenta previa and placenta accreta who had massive life-threatening bleeding during cesarean section: A case report.Medicine (Baltimore). 2019 Apr;98(14):e15025. doi: 10.1097/MD.0000000000015025. Medicine (Baltimore). 2019. PMID: 30946336 Free PMC article.
-
Every minute counts: a network meta-analysis comparing the effect of prophylactic endovascular procedures in abnormal placentation.World J Emerg Surg. 2025 May 24;20(1):43. doi: 10.1186/s13017-025-00602-w. World J Emerg Surg. 2025. PMID: 40413552 Free PMC article.
-
The effect of preoperative intravenous iron administration on patient outcomes in the spectrum of placenta accreta: a retrospective case-control study.BMC Pregnancy Childbirth. 2025 Apr 2;25(1):388. doi: 10.1186/s12884-025-07491-6. BMC Pregnancy Childbirth. 2025. PMID: 40175943 Free PMC article.
References
-
- Silver RM, Landon MB, Rouse DJ, et al. Maternal morbidity associated with multiple repeat Cesarean deliveries. Obstet Gynecol 2006;107:1226–32. - PubMed
-
- Mehrabadi A, Hutcheon JA, Liu S, et al. Contributionof placenta accreta to the incidence of postpartum hemorrhage and severe postpartum hemorrhage. Obstet Gynecol 2015;125:814–21. - PubMed
-
- Thurn L, Lindqvist PG, Jakobsson M, et al. Abnormally invasive placenta-prevalence, risk factors and antenatal suspicion: results from a large population-based pregnancy cohort study in the Nordic countries. BJOG 2016;123:1348–55. - PubMed
-
- Lumbiganon P, Laopaiboon M. Method of delivery and pregnancy outcomes in Asia: the WHO Global Survey on Maternal and Perinatal Health 2007–2008. Lancet 2010;375:490–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
