

Neuroprotection with hypothermia and allopurinol in an animal model of hypoxic-ischemic injury: Is it a gender question?
- PMID: 28931035
- PMCID: PMC5606927
- DOI: 10.1371/journal.pone.0184643
Neuroprotection with hypothermia and allopurinol in an animal model of hypoxic-ischemic injury: Is it a gender question?
Abstract
Background: Hypoxic-ischemic encephalopathy (HIE) is one of the most important causes of neonatal brain injury. Therapeutic hypothermia (TH) is the standard treatment for term newborns after perinatal hypoxic ischemic injury (HI). Despite this, TH does not provide complete neuroprotection. Allopurinol seems to be a good neuroprotector in several animal studies, but it has never been tested in combination with hypothermia. Clinical findings show that male infants with (HI) fare more poorly than matched females in cognitive outcomes. However, there are few studies about neuroprotection taking gender into account in the results. The aim of the present study was to evaluate the potential additive neuroprotective effect of allopurinol when administrated in association with TH in a rodent model of moderate HI. Gender differences in neuroprotection were also evaluated.
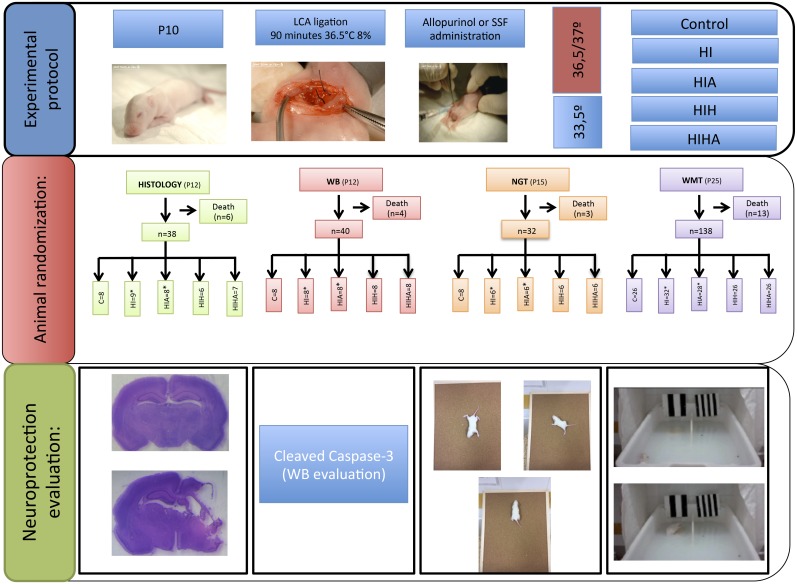
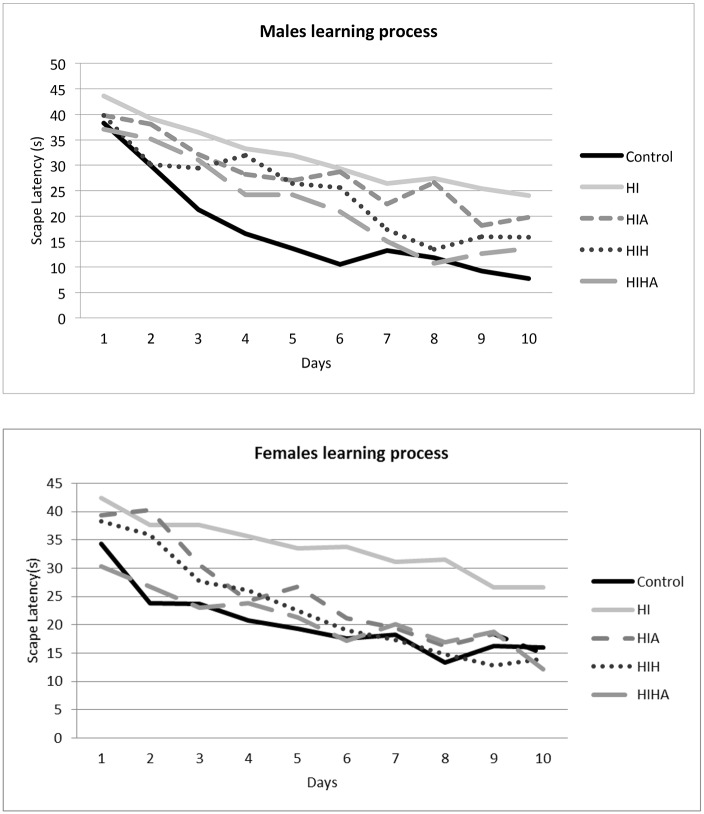
Methods: P10 male and female rat pups were subjected to HI (Vannucci model) and randomized into five groups: sham intervention (Control), no treatment (HI), hypothermia (HIH), allopurinol (HIA), and dual therapy (hypothermia and allopurinol) (HIHA). To evaluate a treatment's neuroprotective efficiency, 24 hours after the HI event caspase3 activation was measured. Damaged area and hippocampal volume were also measured 72 hours after the HI event. Negative geotaxis test was performed to evaluate early neurobehavioral reflexes. Learning and spatial memory were assessed via Morris Water Maze (MWM) test at 25 days of life.
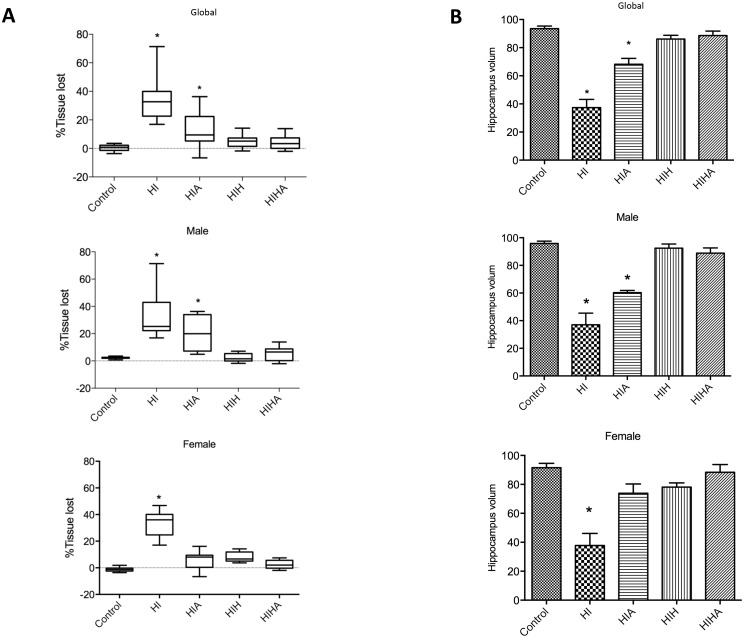
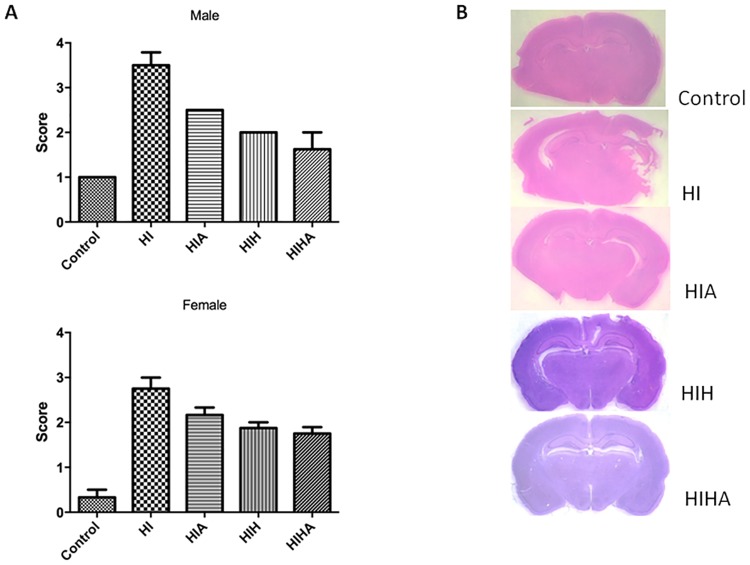
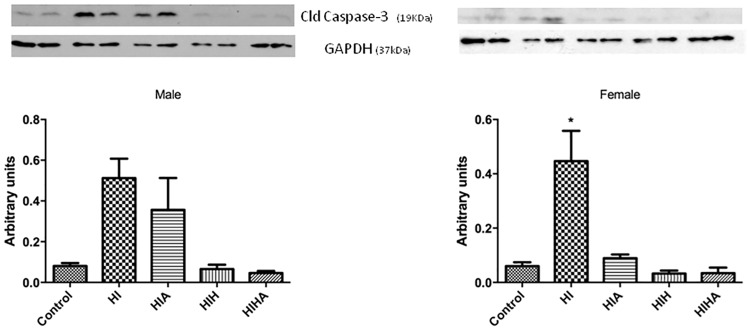
Results: Damaged area and hippocampal volume were different among treatment groups (p = 0.001). The largest tissue lesion was observed in the HI group, followed by HIA. There were no differences between control, HIH, and HIHA. When learning process was analyzed, no differences were found. Females from the HIA group had similar results to the HIH and HIHA groups. Cleaved caspase 3 expression was increased in both HI and HIA. Despite this, in females cleaved caspase-3 was only differently increased in the HI group. All treated animals present an improvement in short-term (Negative geotaxis) and long-term (WMT) functional tests. Despite this, treated females present better long-term outcome. In short-term outcome no sex differences were observed.
Conclusions: Our results suggest that dual therapy confers great neuroprotection after an HI event. There were functional, histological, and molecular improvements in all treated groups. These differences were more important in females than in males. No statistically significant differences were found between HIHA and HIH; both of them present a great improvement. Our results support the idea of different regulation mechanisms and pathways of cell death, depending on gender.
Conflict of interest statement
Figures
References
-
- Smith J, Wells L, Dodd K. The continuing fall in incidence of hypoxic-ischaemic encephalopathy in term infants. BJOG. 2000; 107:461–466. - PubMed
-
- Kurinczuk JJ, White-Koning M, Badawi N. Epidemiology of neonatal encephalopathy and hypoxic-ischaemic encephalopathy. Early Hum Dev. 2010; 86:329–338. doi: 10.1016/j.earlhumdev.2010.05.010 - DOI - PubMed
-
- Glass HC, Ferriero DM. Treatment of hypoxic-ischemic encephalopathy in newborns. Curr Treat Options Neurol. 2007; 9:414–423. - PubMed
-
- Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL, Juszczak E, et al. Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med. 2009; 361:1349–1358. doi: 10.1056/NEJMoa0900854 - DOI - PubMed
-
- Morken TS, Brekke E, Håberg A, Widerøe M, Brubakk AM, Sonnewald U. Altered astrocyte-neuronal interactions after hypoxia-ischemia in the neonatal brain in female and male rats. Stroke. 2014; 45 (9):2777–2785. doi: 10.1161/STROKEAHA.114.005341 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
