

Interleukin-17-positive mast cells influence outcomes from BCG for patients with CIS: Data from a comprehensive characterisation of the immune microenvironment of urothelial bladder cancer
- PMID: 28931051
- PMCID: PMC5607173
- DOI: 10.1371/journal.pone.0184841
Interleukin-17-positive mast cells influence outcomes from BCG for patients with CIS: Data from a comprehensive characterisation of the immune microenvironment of urothelial bladder cancer
Abstract
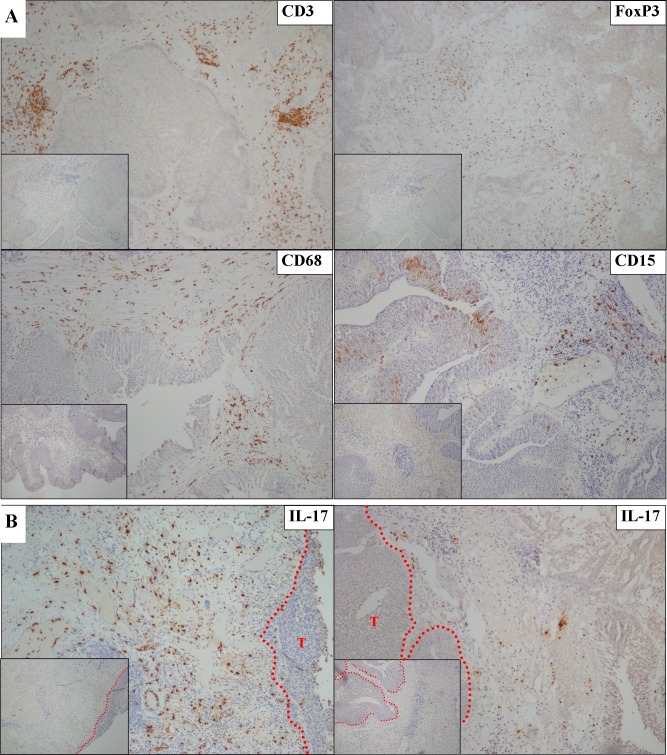
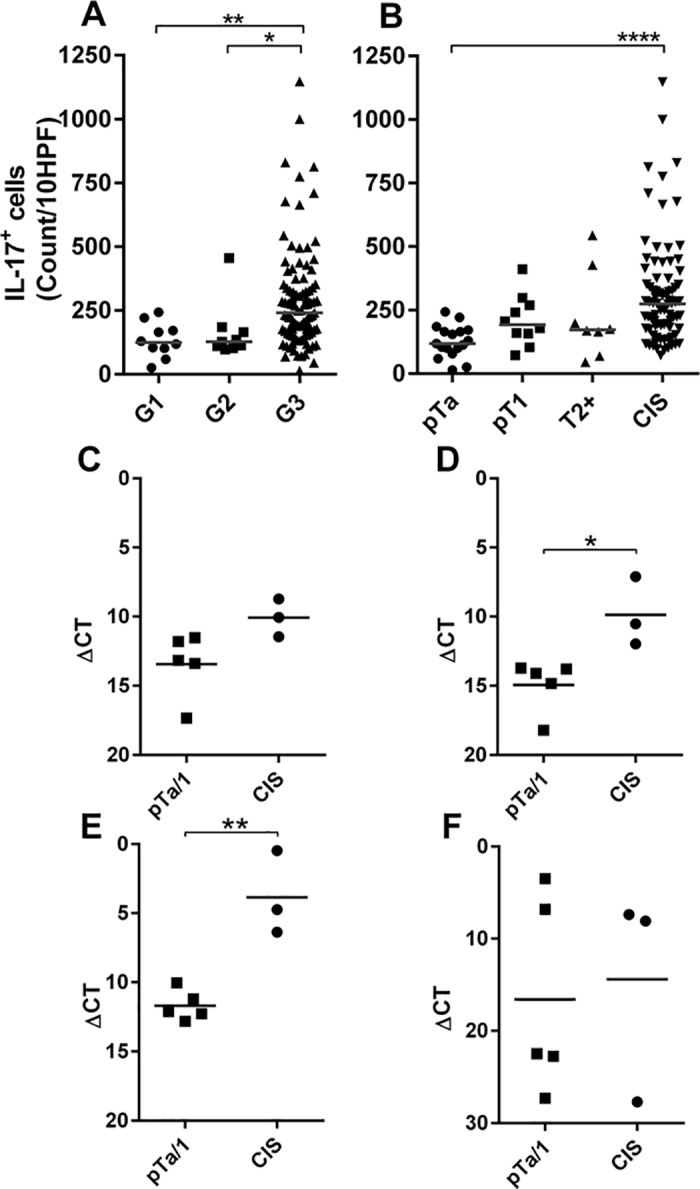
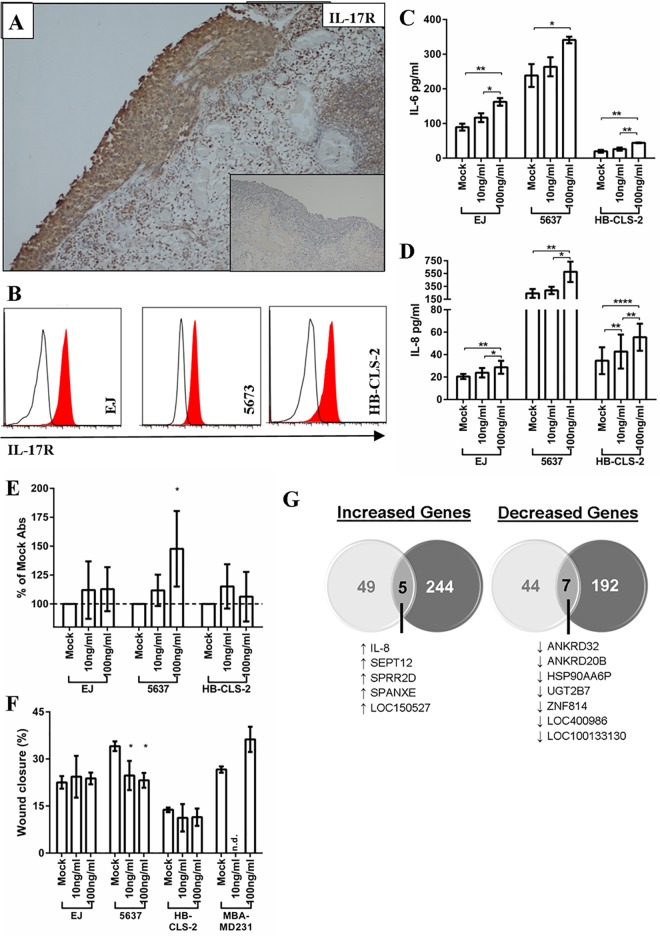
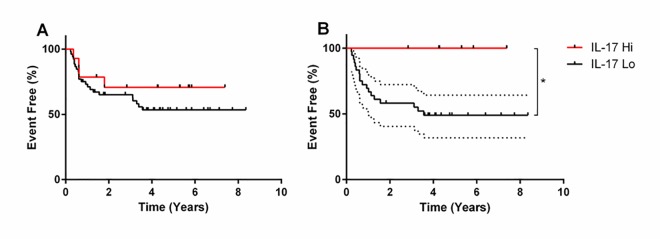
The tumour immune microenvironment is considered to influence cancer behaviour and outcome. Using a panel of markers for innate and adaptive immune cells we set out to characterise and understand the bladder tumour microenvironment of 114 patients from a prospective multicentre cohort of newly-diagnosed bladder cancer patients, followed-up for 4.33±1.71 years. We found IL-17-positive cells were significantly increased in primary and concomitant carcinoma in situ (CIS), p<0.0001, a highly malignant lesion which is the most significant single risk factor for disease progression. Further characterisation of the tumour immunophenotype identified IL-17+ cells as predominantly mast cells rather than T-cells, in contrast to most other tumour types. Expression of the IL-17-receptor in bladder tumours, and functional effects and gene expression changes induced by IL-17 in bladder tumour cells in vitro suggest a role in tumour behaviour. Finally, we assessed the effects of IL-17 in the context of patient outcome, following intravesical BCG immunotherapy which is the standard of care; higher numbers of IL-17+ cells were associated with improved event-free survival (p = 0.0449, HR 0.2918, 95% CI 0.08762-0.9721) in patients with primary and concomitant CIS (n = 41), we propose a model of IL-17+ Mast cells mechanism of action. Thus, in the context of bladder CIS, IL-17+ mast cells predict favourable outcome following BCG immunotherapy indicative of a novel mechanism of BCG immunotherapy in UBC and could form the basis of a stratified approach to treatment.
Conflict of interest statement
Figures


Comment in
-
Bladder cancer: Mastering the immune microenvironment.Nat Rev Urol. 2017 Nov;14(11):639. doi: 10.1038/nrurol.2017.166. Epub 2017 Oct 10. Nat Rev Urol. 2017. PMID: 28994827 No abstract available.
Similar articles
-
Predicting response to bacillus Calmette-Guérin (BCG) in patients with carcinoma in situ of the bladder.Urol Oncol. 2014 Jan;32(1):45.e23-30. doi: 10.1016/j.urolonc.2013.06.008. Epub 2013 Sep 18. Urol Oncol. 2014. PMID: 24055426 Free PMC article.
-
Intravesical treatment of chemotherapeutic agents sensitizes bacillus Calmette‑Guerin by the modulation of the tumor immune environment.Oncol Rep. 2019 Mar;41(3):1863-1874. doi: 10.3892/or.2019.6965. Epub 2019 Jan 10. Oncol Rep. 2019. PMID: 30628699
-
A mathematical model of combined bacillus Calmette-Guerin (BCG) and interleukin (IL)-2 immunotherapy of superficial bladder cancer.J Theor Biol. 2011 May 21;277(1):27-40. doi: 10.1016/j.jtbi.2011.02.008. Epub 2011 Feb 18. J Theor Biol. 2011. PMID: 21334346
-
The role of neutrophils and TNF-related apoptosis-inducing ligand (TRAIL) in bacillus Calmette-Guérin (BCG) immunotherapy for urothelial carcinoma of the bladder.Cancer Metastasis Rev. 2009 Dec;28(3-4):345-53. doi: 10.1007/s10555-009-9195-6. Cancer Metastasis Rev. 2009. PMID: 19967427 Review.
-
Clinical evaluation of immunotherapy: are there differences between papillary and flat in situ bladder cancer?Cancer Surv. 1998;31:99-108. Cancer Surv. 1998. PMID: 15281319 Review.
Cited by
-
Tumor Infiltrating Neutrophils Are Enriched in Basal-Type Urothelial Bladder Cancer.Cells. 2020 Jan 25;9(2):291. doi: 10.3390/cells9020291. Cells. 2020. PMID: 31991796 Free PMC article.
-
Prognostic impact of serum interleukin-6 and 17 level in patients with bladder cancer: a systematic review and meta-analysis.PeerJ. 2025 Apr 29;13:e19385. doi: 10.7717/peerj.19385. eCollection 2025. PeerJ. 2025. PMID: 40321822 Free PMC article.
-
Mast Cell Chymase/Mcpt4 Suppresses the Host Immune Response to Plasmodium yoelii, Limits Malaria-Associated Disruption of Intestinal Barrier Integrity and Reduces Parasite Transmission to Anopheles stephensi.Front Immunol. 2022 Jan 27;13:801120. doi: 10.3389/fimmu.2022.801120. eCollection 2022. Front Immunol. 2022. PMID: 35154114 Free PMC article.
-
Predicting response to bacillus Calmette-Guerin in high-risk non-muscle invasive bladder cancer.Transl Cancer Res. 2024 Nov 30;13(11):6489-6502. doi: 10.21037/tcr-24-180. Epub 2024 Jul 30. Transl Cancer Res. 2024. PMID: 39697728 Free PMC article. Review.
-
Tumor-Associated Mast Cells in Urothelial Bladder Cancer: Optimizing Immuno-Oncology.Biomedicines. 2021 Oct 20;9(11):1500. doi: 10.3390/biomedicines9111500. Biomedicines. 2021. PMID: 34829729 Free PMC article. Review.
References
-
- Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F (2016) Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur Urol. - PubMed
-
- Chavan S, Bray F, Lortet-Tieulent J, Goodman M, Jemal A (2014) International variations in bladder cancer incidence and mortality. Eur Urol 66: 59–73. doi: 10.1016/j.eururo.2013.10.001 - DOI - PubMed
-
- Bryan RT, Zeegers MP, van Roekel EH, Bird D, Grant MR, Dunn JA, et al. (2013) A comparison of patient and tumour characteristics in two UK bladder cancer cohorts separated by 20 years. BJU Int 112: 169–175. doi: 10.1111/bju.12032 - DOI - PubMed
-
- van Rhijn BW, Burger M, Lotan Y, Solsona E, Stief CG, Sylvester RJ, et al. (2009) Recurrence and progression of disease in non-muscle-invasive bladder cancer: from epidemiology to treatment strategy. Eur Urol 56: 430–442. doi: 10.1016/j.eururo.2009.06.028 - DOI - PubMed
-
- Riley GF, Potosky AL, Lubitz JD, Kessler LG (1995) Medicare payments from diagnosis to death for elderly cancer patients by stage at diagnosis. Med Care 33: 828–841. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
