

Acute HIV infection presenting as hemophagocytic lymphohistiocytosis: case report and review of the literature
- PMID: 28931369
- PMCID: PMC5607499
- DOI: 10.1186/s12879-017-2732-y
Acute HIV infection presenting as hemophagocytic lymphohistiocytosis: case report and review of the literature
Abstract
Background: Hemophagocytic lymphohistiocytosis (HLH) is an uncommon systemic inflammatory condition that can result from infections, autoimmune diseases and malignancies. It is a rarely reported life threatening complication of an acute HIV infection, with only ten documented case reports per our literature search. We present a case of HLH secondary to acute HIV infection with a negative HIV antibody-based assay and high plasma viral load.
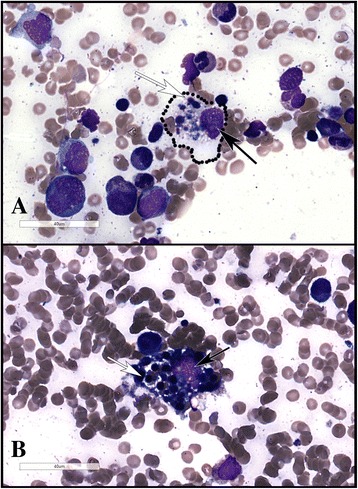
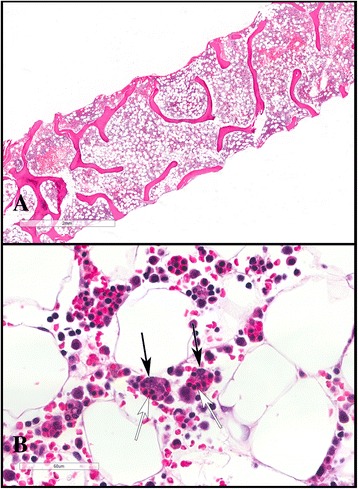
Case presentation: A 45 year old male with a past medical history of well controlled hypertension presented with fever, dizziness and non-bloody diarrhea. Initial lab work revealed a new thrombocytopenia, marked renal failure and an elevated creatine kinase, ferritin, lactate dehydrogenase and D-dimer. A bone marrow biopsy revealed HLH. As part of the work up for thrombocytopenia, a rapid HIV antibody based assay was done and was negative. The sample was later routinely tested with a fourth generation antigen/antibody assay as per local protocol and was strongly positive. The plasma RNA viral load was >10,000,000 copies /mL confirming the diagnosis of an acute HIV infection. The patient was urgently started on antiretroviral therapy and recovered.
Conclusion: This case illustrates a diagnostic approach to HLH which is an uncommon but life threatening multisystem disease, requiring the involvement of a multidisciplinary team of experts. Following any diagnosis of HLH, rapid identification and treatment of the underlying condition is critical. A negative rapid HIV antibody test can be misleading in the context of early HIV infection and the additional use of fourth generation antigen/antibody test or plasma RNA viral load may be required within the right clinical context for diagnosis.
Keywords: Acute retroviral syndrome; HIV; Hemophagocytic lymphohistiocytosis; Hemophagocytic syndrome; Human immunodeficiency virus.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Consent has been obtained from the patient for the publishing of this case report and any accompanying data. Additionally, consent has been obtained for the publishing of images from his bone marrow biopsy. This consent has been explicitly documented in the patient’s clinical chart.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
HIV infection presenting proliferation of CD8+ T lymphocyte and hemophagocytic lymphohistiocytosis.Int J STD AIDS. 2016 Apr;27(5):411-3. doi: 10.1177/0956462415585254. Epub 2015 May 4. Int J STD AIDS. 2016. PMID: 25941054
-
An Unusual Case of Hemophagocytic Lymphohistiocytosis Presentation in Acute Human Immunodeficiency Virus.J Investig Med High Impact Case Rep. 2021 Jan-Dec;9:23247096211021696. doi: 10.1177/23247096211021696. J Investig Med High Impact Case Rep. 2021. PMID: 34078147 Free PMC article.
-
Hemophagocytic Lymphohistiocytosis in Renal Transplant Recipients: A 2-Case Report.Transplant Proc. 2020 Jun;52(5):1566-1569. doi: 10.1016/j.transproceed.2020.02.047. Epub 2020 May 8. Transplant Proc. 2020. PMID: 32389490
-
Acquired hemophagocytic lymphohistiocytosis as initial manifestation of multiple myeloma: A case report and literature review.Medicine (Baltimore). 2020 Sep 25;99(39):e22299. doi: 10.1097/MD.0000000000022299. Medicine (Baltimore). 2020. PMID: 32991435 Free PMC article. Review.
-
Hemophagocytic Lymphohistiocytosis mimics many common conditions: case series and review of literature.Eur Ann Allergy Clin Immunol. 2017 Jan;49(1):31-41. Eur Ann Allergy Clin Immunol. 2017. PMID: 28120605 Review.
Cited by
-
Tuberculosis-Associated HLH in an 8-Month-Old Infant: A Case Report and Review.Front Pediatr. 2020 Oct 30;8:556155. doi: 10.3389/fped.2020.556155. eCollection 2020. Front Pediatr. 2020. PMID: 33194891 Free PMC article.
-
Hemophagocytic Lymphohistiocytosis and Hodgkin Lymphoma in a Newly Diagnosed HIV Patient: A Diagnostic Dilemma.Cureus. 2023 Jun 29;15(6):e41127. doi: 10.7759/cureus.41127. eCollection 2023 Jun. Cureus. 2023. PMID: 37519529 Free PMC article.
-
Cytokine Storm Syndrome as a Manifestation of Primary HIV Infection.Adv Exp Med Biol. 2024;1448:269-274. doi: 10.1007/978-3-031-59815-9_18. Adv Exp Med Biol. 2024. PMID: 39117820 Review.
-
The Predictive Value of Lactate Dehydrogenase for Viral Suppression in Newly Diagnosed People Living With HIV on Antiretroviral Therapy: A Retrospective Cohort Study.Infect Drug Resist. 2025 Jan 30;18:601-611. doi: 10.2147/IDR.S488220. eCollection 2025. Infect Drug Resist. 2025. PMID: 39902274 Free PMC article.
-
Hemophagocytic lymphohistiocytosis following an acute HIV infection, in a known immunosuppressed patient: A case report.IDCases. 2022 Jun 15;29:e01534. doi: 10.1016/j.idcr.2022.e01534. eCollection 2022. IDCases. 2022. PMID: 35785038 Free PMC article.
References
-
- Cascio A, Pernice LM, Barberi G, Delfino D, Biondo C, Beninati C, Mancuso G, Rodriguez-Morales AJ, Iaria C. Secondary hemophagocytic lymphohistiocytosis in zoonoses. A systematic review. Eur Rev Med Pharmacol Sci. 2012;16(10):1324–1337. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
