

The rehabilitation enhancing aging through connected health (REACH) study: study protocol for a quasi-experimental clinical trial
- PMID: 28931377
- PMCID: PMC5607604
- DOI: 10.1186/s12877-017-0618-x
The rehabilitation enhancing aging through connected health (REACH) study: study protocol for a quasi-experimental clinical trial
Abstract
Background: Mobility limitations among older adults increase the risk for disability and healthcare utilization. Rehabilitative care is identified as the most efficacious treatment for maintaining physical function. However, there is insufficient evidence identifying a healthcare model that targets prevention of mobility decline among older adults. The objective of this study is to evaluate the preliminary effectiveness of a physical therapy program, augmented with mobile tele-health technology, on mobility function and healthcare utilization among older adults.
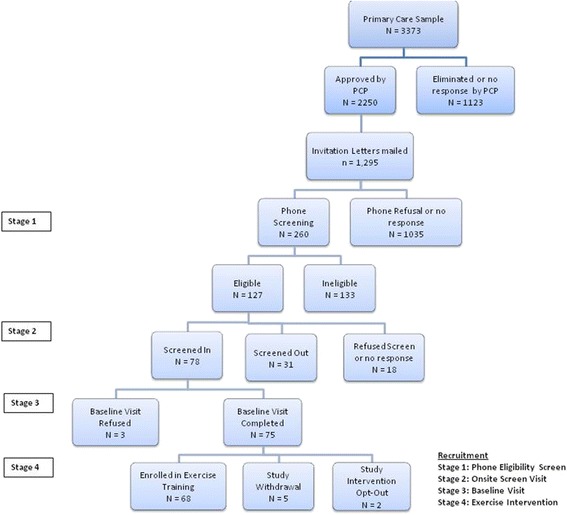
Methods: This is a quasi-experimental 12-month clinical trial conducted within a metropolitan-based healthcare system in the northeastern United States. It is in parallel with an existing longitudinal cohort study evaluating mobility decline among community-dwelling older adult primary care patients over one year. Seventy-five older adults (≥ 65-95 years) are being recruited using identical inclusion/exclusion criteria to the cohort study. Three aims will be evaluated: the effect of our program on 1) physical function, 2) healthcare utilization, and 3) healthcare costs. Changes in patient-reported function over 1 year in those receiving the intervention (aim 1) will be compared to propensity score matched controls (N = 150) from the cohort study. For aims 2 and 3, propensity scores, derived from logistic regression model that includes demographic and diagnostic information available through claims and enrollment information, will be used to match treatment and control patients in a ratio of 1:2 or 1:3 from a Medicare Claims Registry derived from the same geographic region. The intervention consists of a one-year physical therapy program that is divided between a combination of outpatient and home visits (6-10 total visits) and is augmented on a computerized tablet using of a commercially available application to deliver a progressive home-based exercise program emphasizing lower-extremity function and a walking program.
Discussion: Incorporating mobile health into current healthcare models of rehabilitative care has the potential to decrease hospital visits and provide a longer duration of care. If the hypotheses are supported and demonstrate improved mobility and reduced healthcare utilization, this innovative care model would be applicable for optimizing the maintenance of functional independence among community-dwelling older adults.
Trial registration: ClinicalTrial.gov Identifier: NCT02580409 (Date of registration October 14, 2015).
Keywords: Geriatrics; Healthcare model; Mobility; Physical therapy.
Conflict of interest statement
Ethics approval and consent to participate
The current study and the Boston RISE study are approved by the Spaulding Rehabilitation Hospital Research Ethics Committee. Participants were given informed consent before taking part.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Boyd CM, Leff B, Wolff JL, Yu Q, Zhou J, Rand C, et al. Informing clinical practice guideline development and implementation: prevalence of coexisting conditions among adults with coronary heart disease. J Am Geriatr Soc. 2011;59(5):797–805. doi: 10.1111/j.1532-5415.2011.03391.x. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
