

Evaluating a preoperative protocol that includes magnetic resonance imaging for lymph node metastasis in the Cholangiocarcinoma Screening and Care Program (CASCAP) in Thailand
- PMID: 28931405
- PMCID: PMC5607577
- DOI: 10.1186/s12957-017-1246-9
Evaluating a preoperative protocol that includes magnetic resonance imaging for lymph node metastasis in the Cholangiocarcinoma Screening and Care Program (CASCAP) in Thailand
Abstract
Background: Treatment planning especially liver resection in cholangiocarcinoma (CCA) depends on the extension of tumor and lymph node metastasis which is included as a key criterion for operability. Magnetic resonance imaging (MRI) offers a rapid and powerful tool for the detection of lymph node metastasis (LNM) and in the current manuscript is assessed as a critical tool in the preoperative protocol for liver resection for treatment of CCA. However, the accuracy of MRI to detect LNM from CCA had yet to be comprehensively evaluated.
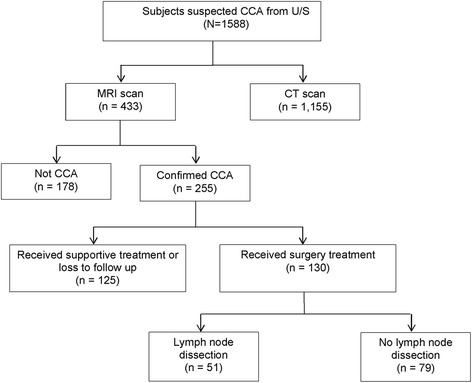
Methods: The accuracy of MRI to detect LNM was assessed in a cohort of individuals with CCA from the Cholangiocarcinoma Screening and Care Program (CASCAP), a screening program designed to reduce CCA in Northeastern Thailand by community-based ultrasound (US) for CCA. CCA-positive individuals are referred to one of the nine tertiary centers in the study to undergo a preoperative protocol that included enhanced imaging by MRI. Additionally, these individuals also underwent lymph node biopsies for histological confirmation of LNM (the "gold standard") to determine the accuracy of the MRI results.
Results: MRI accurately detected the presence or absence of LNM in only 29 out of the 51 CCA cases (56.9%, 95% CI 42.2-70.7), resulting in a sensitivity of 57.1% (95% CI 34.0-78.2) and specificity of 56.7% (95% CI 37.4-74.5), with positive and negative predictive values of 48.0% (95% CI 27.8-68.7) and 65.4% (95% CI 44.3-82.8), respectively. The positive likelihood ratio was 1.32 (95% CI 0.76-2.29), and the negative likelihood ratio was 0.76 (95% CI 0.42-1.36).
Conclusions: MRI showed limited sensitivity and a poor positive predictive value for the diagnosis of LNM for CCA, which is of particular concern in this resource-limited setting, where simpler detection methods could be utilized that are more cost-effective in this region of Thailand. Therefore, the inclusion of MRI, a costly imaging method, should be reconsidered as part of protocol for treatment planning of CCA, given the number of false positives, especially as it is critical in determining the operability for CCA subjects.
Keywords: Accuracy; Cholangiocarcinoma; Lymph node metastasis; Magnetic resonance imaging; Preoperative protocol.
Conflict of interest statement
Consent for publication
The patients were informed that the data concerning the case would be submitted for publication and they consented.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Preoperative criterion identifying a low-risk group for lymph node metastasis in intrahepatic cholangiocarcinoma.J Hepatobiliary Pancreat Sci. 2018 Jun;25(6):299-307. doi: 10.1002/jhbp.552. Epub 2018 May 22. J Hepatobiliary Pancreat Sci. 2018. PMID: 29656560
-
Prognostic Impact of Preoperative Lymph Node Enlargement in Intrahepatic Cholangiocarcinoma: A Multi-Institutional Study by the Kyushu Study Group of Liver Surgery.Ann Surg Oncol. 2015 Jul;22(7):2269-78. doi: 10.1245/s10434-014-4239-8. Epub 2015 Jan 13. Ann Surg Oncol. 2015. PMID: 25582737
-
Clinical role of 18F-FDG PET-CT in suspected and potentially operable cholangiocarcinoma: a prospective study compared with conventional imaging.Am J Gastroenterol. 2008 May;103(5):1145-51. doi: 10.1111/j.1572-0241.2007.01710.x. Epub 2008 Jan 2. Am J Gastroenterol. 2008. PMID: 18177454
-
Multidetector computed tomography in the preoperative workup of hilar cholangiocarcinoma.Acta Radiol. 2009 Oct;50(8):845-53. doi: 10.1080/02841850903092366. Acta Radiol. 2009. PMID: 19639473 Review.
-
Lymph node dissection for intrahepatic cholangiocarcinoma: a critical review of the literature to date.J Hepatobiliary Pancreat Sci. 2014 Mar;21(3):162-8. doi: 10.1002/jhbp.30. Epub 2013 Sep 11. J Hepatobiliary Pancreat Sci. 2014. PMID: 24027075 Review.
Cited by
-
Personalized intrahepatic cholangiocarcinoma prognosis prediction using radiomics: Application and development trend.Front Oncol. 2023 Mar 23;13:1133867. doi: 10.3389/fonc.2023.1133867. eCollection 2023. Front Oncol. 2023. PMID: 37035147 Free PMC article. Review.
-
Prognostic Value of Lymph Node Dissection for Intrahepatic Cholangiocarcinoma Patients With Clinically Negative Lymph Node Metastasis: A Multi-Center Study From China.Front Oncol. 2021 Mar 11;11:585808. doi: 10.3389/fonc.2021.585808. eCollection 2021. Front Oncol. 2021. PMID: 33777738 Free PMC article.
-
Cholangiocarcinoma: anatomical location-dependent clinical, prognostic, and genetic disparities.Ann Transl Med. 2019 Dec;7(23):744. doi: 10.21037/atm.2019.12.37. Ann Transl Med. 2019. PMID: 32042760 Free PMC article.
-
Apparent diffusion coefficient value of mass-forming intrahepatic cholangiocarcinoma: a potential imaging biomarker for prediction of lymph node metastasis.Abdom Radiol (NY). 2020 Oct;45(10):3109-3118. doi: 10.1007/s00261-020-02458-x. Abdom Radiol (NY). 2020. PMID: 32107582
-
Contrast-Enhanced Imaging in the Management of Intrahepatic Cholangiocarcinoma: State of Art and Future Perspectives.Cancers (Basel). 2023 Jun 28;15(13):3393. doi: 10.3390/cancers15133393. Cancers (Basel). 2023. PMID: 37444503 Free PMC article. Review.
References
-
- Green A, Uttaravichien T, Bhudhisawasdi V, Chartbanchachai W, Elkins DB, Marieng EO, et al. Cholangiocarcinoma in north east Thailand. A hospital-based study. Trop Geogr Med. 1991;43(1–2):193–198. - PubMed
-
- Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 7-14 June 1994. IARC Monogr Eval Carcinog Risks Hum. 1994;61:1-241. http://www.ncbi.nlm.nih.gov/pubmed/7715068. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
