

Serum 1,5-anhydroglucitol when used with fasting plasma glucose improves the efficiency of diabetes screening in a Chinese population
- PMID: 28931928
- PMCID: PMC5607288
- DOI: 10.1038/s41598-017-12210-z
Serum 1,5-anhydroglucitol when used with fasting plasma glucose improves the efficiency of diabetes screening in a Chinese population
Abstract
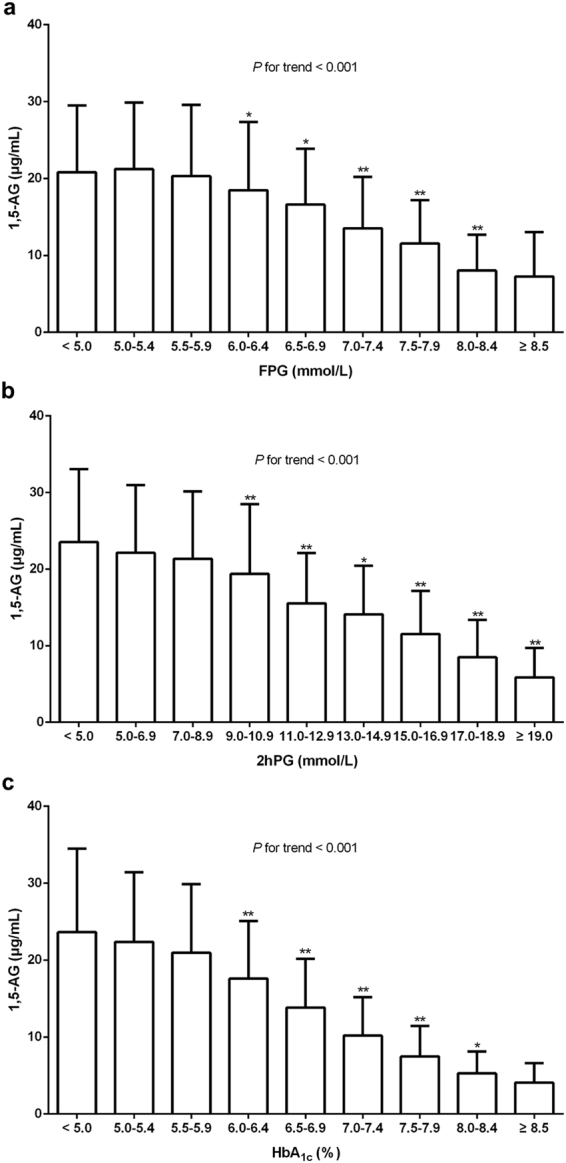
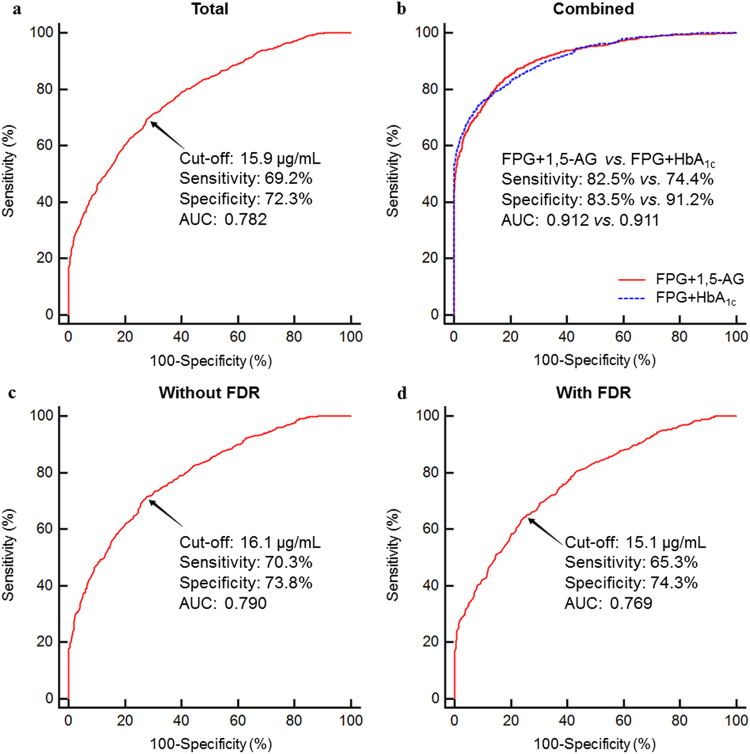
Serum 1,5-anhydroglucitol (1,5-AG) levels can not only accurately reflect the mean blood glucose over the previous 1-2 weeks in diabetic patients but also offers the advantage of representing postprandial glucose. To evaluate the clinical significance of 1,5-AG in diabetes detection, especially when used in combination with fasting plasma glucose (FPG), a total of 3098 participants at high risk for diabetes (1467 men, 1631 women) were enrolled. A total of 1471 (47.5%) participants were diagnosed with diabetes, and the mean 1,5-AG level in the diabetic group was significantly lower than that in non-diabetic group [12.5 (7.8-17.5) μg/mL vs. 20.5 (15.3-26.4) μg/mL, P < 0.001]. The optimal cut-off point was 15.9 μg/mL, for which the sensitivity, specificity, and area under the curve (AUC) were 69.2%, 72.3%, and 0.781, respectively. For the combination of FPG and 1,5-AG, the sensitivity, specificity, and AUC improved to 82.5%, 83.5%, and 0.912, respectively. This method helped 75.8% of the participants avoid an oral glucose tolerance test (OGTT), reducing the need to carry out the OGTT by 43.9% compared to the use of the FPG criterion only. In conclusion, the addition of FPG to serum 1,5-AG improves the efficiency of diabetes screening in the Chinese population.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Li L, Jick S, Breitenstein S, Michel A. Prevalence of diabetes and diabetic nephropathy in a large U.S. commercially insured pediatric population, 2002–2013. Diabetes Care. 2016;39:278–284. - PubMed
-
- Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15:539–553. doi: 10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
