

Body surface area: a novel predictor for conversion to thoracotomy in patients undergoing video-assisted thoracoscopic lung cancer lobectomy
- PMID: 28932543
- PMCID: PMC5594169
- DOI: 10.21037/jtd.2017.07.53
Body surface area: a novel predictor for conversion to thoracotomy in patients undergoing video-assisted thoracoscopic lung cancer lobectomy
Abstract
Background: The purpose of our study was to explore the value of body surface area (BSA) for predicting conversion to thoracotomy in patients undergoing video-assisted thoracoscopic (VATS) lobectomy for non-small cell lung cancer (NSCLC).
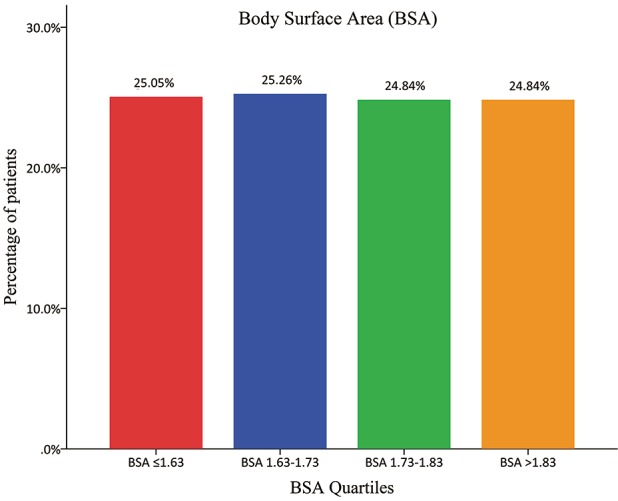
Methods: We performed a monocentric retrospective analysis based on a prospectively-maintained dataset of consecutive patients between March 2014 and August 2015 at our unit. The median value of BSA was used as the cut-off. Patients with BSA > median value were classified as the "large" group, while those with BSA ≤ median value were classified as the "non-large" group. The conversion rate and post-VATS morbidity between these two groups were evaluated. Finally, a multivariate logistic-regression analysis was performed to identify the predictors for conversion to thoracotomy.
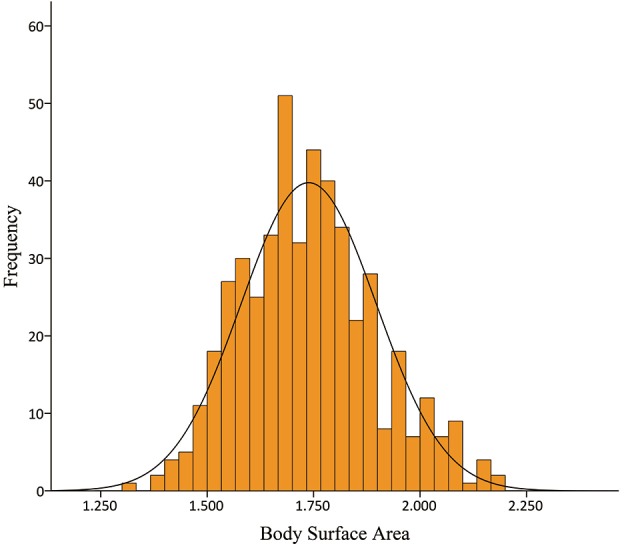
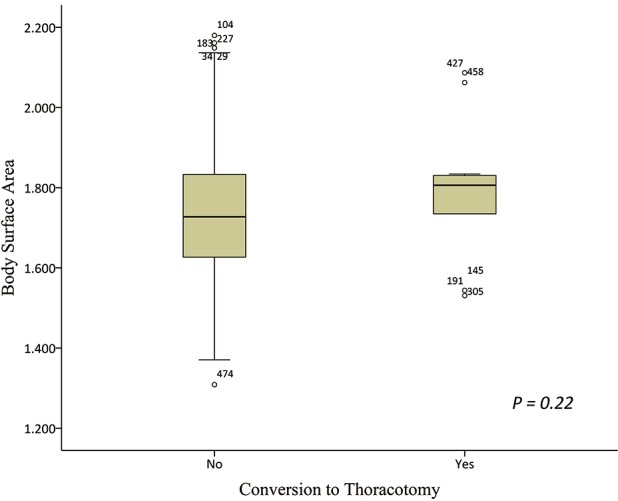
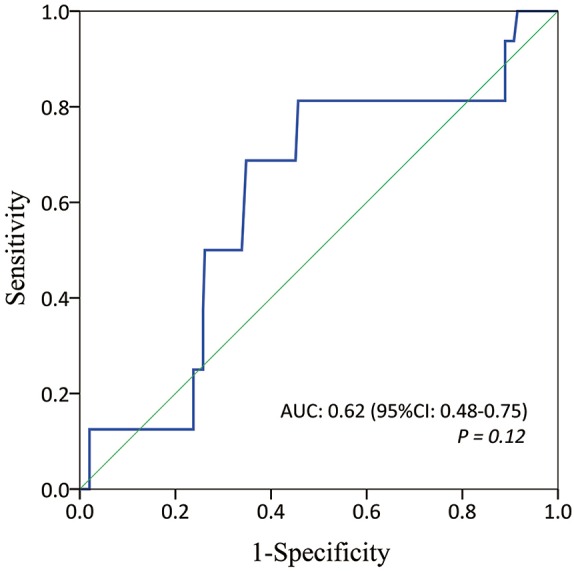
Results: A total of 475 patients with a median BSA of 1.73 m2 were enrolled. There were 16 patients converted to thoracotomy (ratio =3.4%). The overall morbidity rate was 28.4%. The "large" group (BSA >1.73 m2) included 236 patients, while the "non-large" group (BSA ≤1.72 m2) included the remaining 239 patients. The conversion (5.5% vs. 1.3%; P=0.010) in the "large" patients was significantly higher than that in the "non-large" patients. No difference was found in the overall morbidity rate between these two groups (32.2% vs. 24.7%; P=0.069). The multivariate logistic-regression analysis demonstrated that BSA >1.73 m2 could be a strongly independent predictor for conversion to thoracotomy [odds ratio (OR): 7.17; P=0.028].
Conclusions: BSA is an excellent categorical predictor for conversion to thoracotomy in NSCLC patients undergoing VATS lobectomy. It may be considered when informing patients about intraoperative risks and selecting cases in the early learning curve of VATS techniques.
Keywords: Body surface area (BSA); conversion to thoracotomy; lobectomy; video-assisted thoracoscopic surgery (VATS).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Li S, Wang Z, Huang J, et al. Systematic review of prognostic roles of body mass index for patients undergoing lung cancer surgery: does the 'obesity paradox' really exist? Eur J Cardiothorac Surg 2017;51:817-28. - PubMed
-
- Roviaro G, Rebuffat C, Varoli F, et al. Videoendoscopic pulmonary lobectomy for cancer. Surg Laparosc Endosc 1992;2:244-7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources