

Correlation between EGFR mutation status and the incidence of brain metastases in patients with non-small cell lung cancer
- PMID: 28932557
- PMCID: PMC5594201
- DOI: 10.21037/jtd.2017.07.57
Correlation between EGFR mutation status and the incidence of brain metastases in patients with non-small cell lung cancer
Abstract
Background: Lung cancer is the leading cause of cancer-related death worldwide. Numerous studies have been performed to investigate the correlation between epidermal growth factor receptor (EGFR) mutation status and the incidence of brain metastases (BMs) in patients with non-small cell lung cancer (NSCLC), however, the outcomes were inconsistent. Thus, we performed this study to establish the role of EGFR mutation status in BMs.
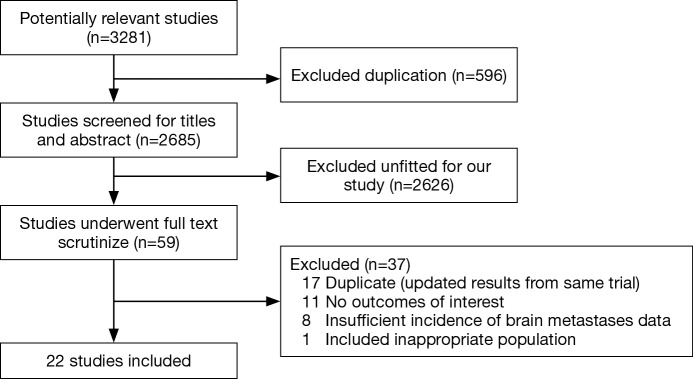
Methods: Electronic databases PubMed, Embase, Cochrane Library, CBM, WanFang, CNKI were searched to identify relevant trials. The primary endpoint was the incidence of BMs in EGFR mutations or wild type NSCLC and the secondary endpoint was overall survival calculated from the BMs emerging (BMOS).
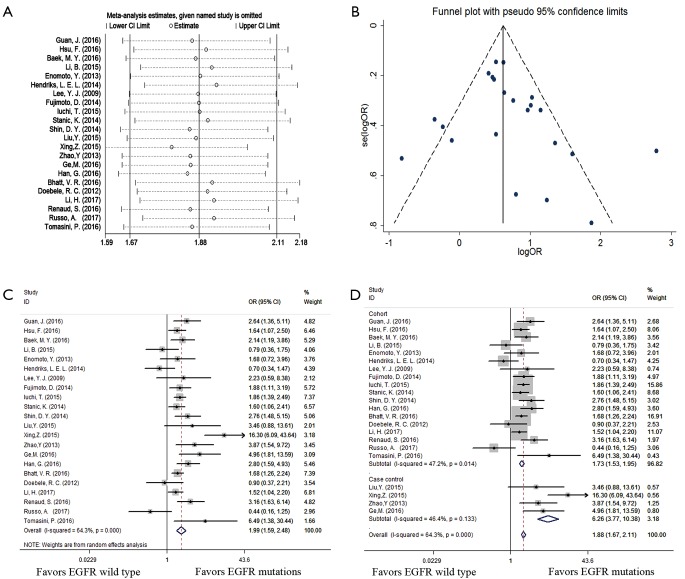
Results: Twenty-two studies incorporating 8,152 participants were eligible. EGFR mutations group possessed a significantly higher risk of BMs (OR =1.99; 95% CI, 1.59-2.48; P=0.000) than EGFR wild type group. In the stratified analysis, compared with EGFR wild type group, EGFR mutations group had a significant higher incidence (OR =2.01; 95% CI, 1.56-2.59; P=0.000) of subsequent BMs while only a trend of increasing the incidence of initial BMs (OR =1.38; 95% CI, 0.98-1.94; P=0.066). Moreover, exon 19 deletion had a trend of increasing the incidence of BMs than exon 21 mutation (OR =1.44; 95% CI, 0.77-2.68; P=0.252). Compared with EGFR wild type group, EGFR mutations group possessed a prolonged overall BMOS (HR =0.68; 95% CI, 0.47-0.98; P=0.038) and a longer BMOS in initial BMs (HR =0.50; 95% CI, 0.31-0.80; P=0.004) but no significant difference in NSCLC with subsequent BMs (HR =0.95; 95% CI, 0.42-2.15; P=0.901).
Conclusions: Patients with EGFR mutations were more susceptible to develop into BMs than those with EGFR wild type, especially during the course of disease.
Keywords: Brain metastases (BMs); epidermal growth factor receptor (EGFR); meta-analysis; non-small cell lung cancer (NSCLC).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous