

The technique of endoscopic airway tumor treatment
- PMID: 28932570
- PMCID: PMC5594167
- DOI: 10.21037/jtd.2017.07.68
The technique of endoscopic airway tumor treatment
Abstract
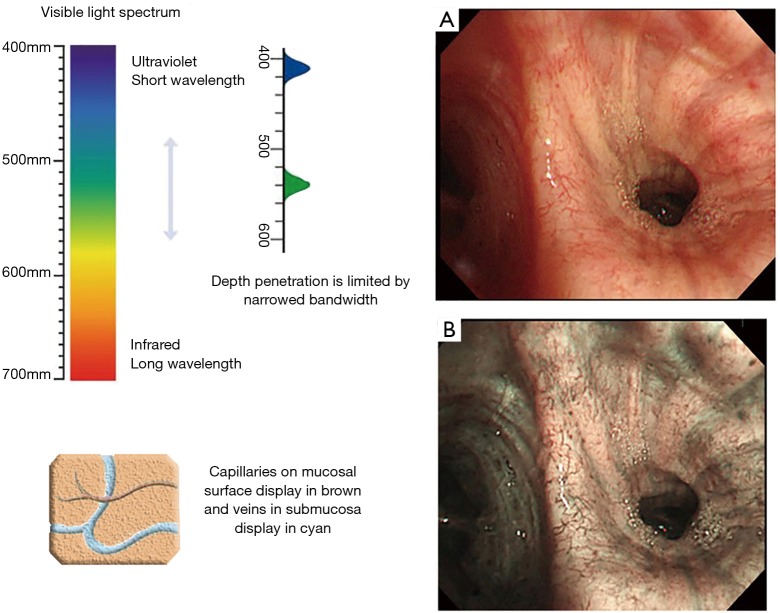
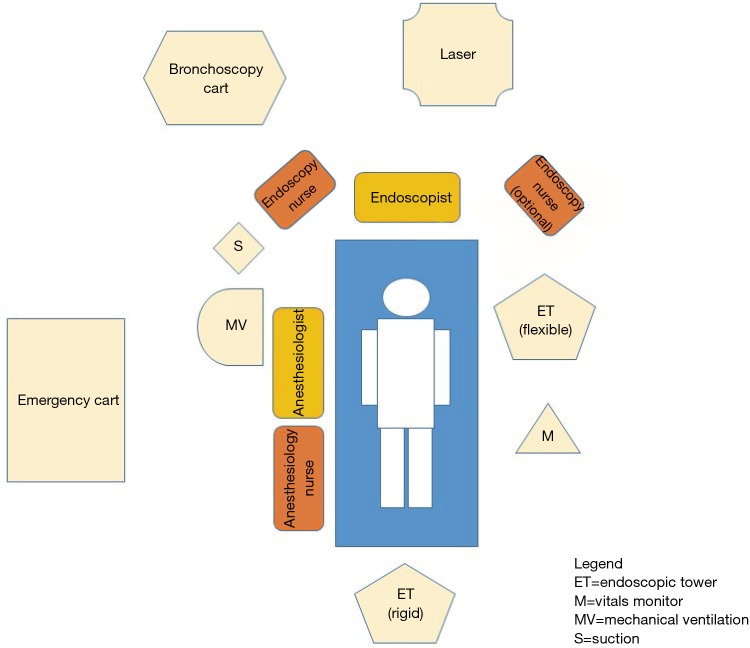
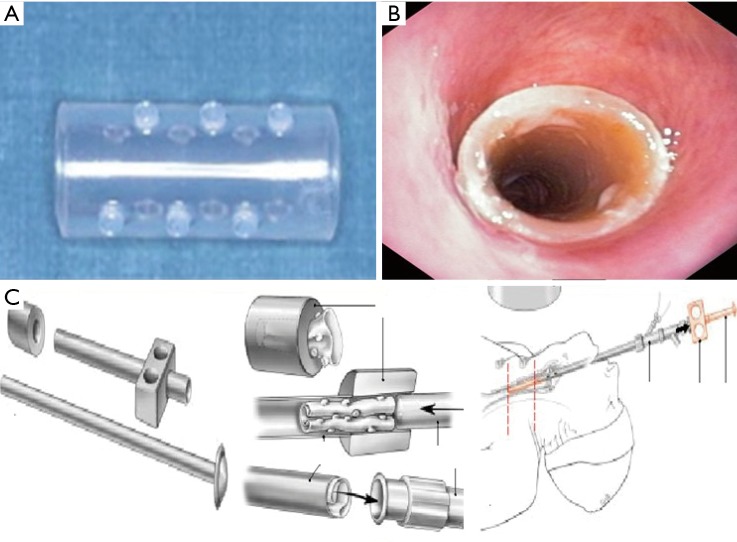
More than half of primary lung cancers are not resectable at diagnosis and 40% of deaths may be secondary to loco-regional disease. Many of these patients suffer from symptoms related to airways obstruction. Indications for therapeutic endoscopic treatment are palliation of dyspnea and other obstructive symptoms in advanced cancerous lesions and cure of early lung cancer. Bronchoscopic management is also indicated for all those patients suffering from benign or minimally invasive neoplasm who are not suitable for surgery due to their clinical conditions. Clinicians should select cases, evaluating tumor features (size, location) and patient characteristics (age, lung function impairment) to choose the most appropriate endoscopic technique. Laser therapy, electrocautery, cryotherapy and stenting are well-described techniques for the palliation of symptoms due to airway involvement and local treatment of endobronchial lesions. Newer technologies, with an established role in clinical practice, are endobronchial ultrasound (EBUS), autofluorescence bronchoscopy (AFB), and narrow band imaging (NBI). Other techniques, such as endobronchial intra-tumoral chemotherapy (EITC), EBUS-guided-transbronchial needle injection or bronchoscopy-guided radiofrequency ablation (RFA), are in development for the use within the airways. These endobronchial interventions are important adjuncts in the multimodality management of lung cancer and should become standard considerations in the management of patients with advanced lung cancer, benign or otherwise not approachable central airway lesions. We aimed at revising several endobronchial treatment modalities that can augment standard antitumor therapies for advanced lung cancer, including rigid and flexible bronchoscopy, laser therapy, endobronchial prosthesis, and photodynamic therapy (PDT).
Keywords: Interventional pulmonology; lung cancer; tracheo-bronchial malignancies; tracheobronchial endoscopy; treatment.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures



References
-
- Cancer Research UK. Lung cancer incidence statistics. Date last accessed: January 3, 2015. Date last updated: May 29, 2014. Available online: www.cancerresearchuk.org/cancer-info/cancerstats/types/lung/incidence/uk...
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources