

Chronic lung allograft dysfunction phenotypes and treatment
- PMID: 28932572
- PMCID: PMC5594185
- DOI: 10.21037/jtd.2017.07.81
Chronic lung allograft dysfunction phenotypes and treatment
Abstract
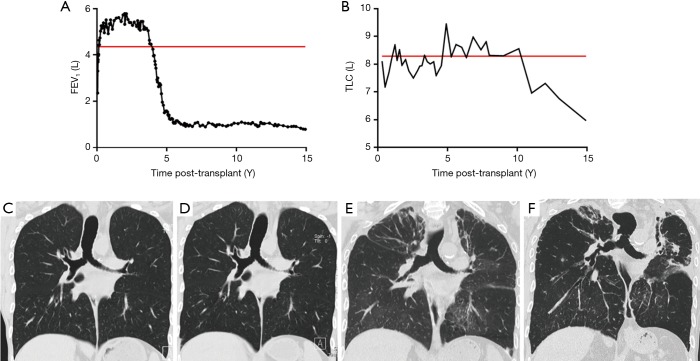
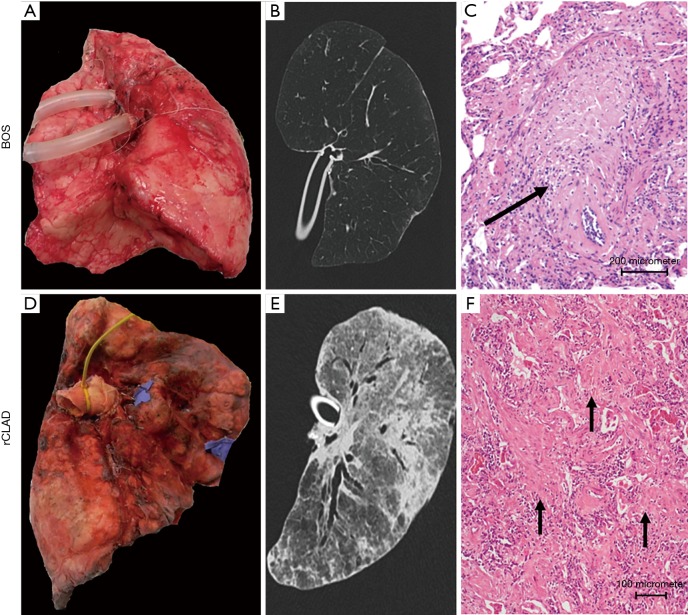
Chronic lung allograft dysfunction (CLAD) remains a major hurdle limiting long-term survival post lung transplantation. Given the clinical heterogeneity of CLAD, recently two phenotypes of CLAD have been defined [bronchiolitis obliterans syndrome (BOS) vs. restrictive allograft syndrome (RAS) or restrictive CLAD (rCLAD)]. BOS is characterized by an obstructive pulmonary function, air trapping on CT and obliterative bronchiolitis (OB) on histopathology, while RAS/rCLAD patients show a restrictive pulmonary function, persistent pleuro-parenchymal infiltrates on CT and pleuroparenchymal fibro-elastosis on biopsies. Importantly, the patients with RAS/rCLAD have a severely limited survival post diagnosis of 6-18 months compared to 3-5 years after BOS diagnosis. In this review, we will review historical evidence for this heterogeneity and we will highlight the clinical, radiological, histopathological characteristics of both phenotypes, as well as their risk factors. Treatment of CLAD remains troublesome, nevertheless, we will give an overview of different treatment strategies that have been tried with some success. Adequate phenotyping remains difficult but is clearly needed for both clinical and scientific purposes.
Keywords: Lung transplantation; bronchiolitis obliterans syndrome (BOS); chronic lung allograft dysfunction (CLAD); chronic rejection; restrictive allograft syndrome (RAS).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Yusen RD, Edwards LB, Dipchand AI, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Lung and Heart-Lung Transplant Report-2016; Focus Theme: Primary Diagnostic Indications for Transplant. J Heart Lung Transplant 2016;35:1170-84. 10.1016/j.healun.2016.09.001 - DOI - PubMed
-
- Chamberlain D, Maurer J, Chaparro C, et al. Evaluation of transbronchial lung biopsy specimens in the diagnosis of bronchiolitis obliterans after lung transplantation. J Heart Lung Transplant 1994;13:963-71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous