

Benign superior vena cava syndrome with uncontrolled pleural effusion by calcified mediastinal lymphadenopathy: surgical management
- PMID: 28932580
- PMCID: PMC5594184
- DOI: 10.21037/jtd.2017.06.51
Benign superior vena cava syndrome with uncontrolled pleural effusion by calcified mediastinal lymphadenopathy: surgical management
Abstract
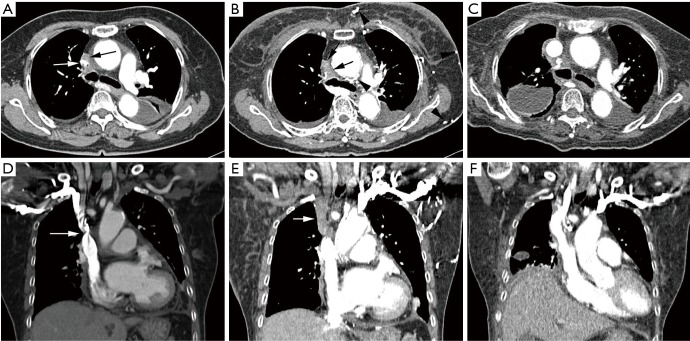
This report describes a rare case of benign superior vena cava syndrome (SVCS) accompanying recalcitrant pleural effusion developed secondary to extrinsic compression by anthracotic calcified mediastinal lymphadenopathy which was corrected by surgical bypass graft. An 81-year-old female presented with recalcitrant pleural effusion for several months despite of medical treatments. SVCS developed progressively without any other radiological evidence of malignancy or active infection on initial chest computed tomography (CT). A follow-up chest CT scan taken one month later revealed a poorly-defined mass-like lesion encasing the SVC. Near total collapse of the SVC due to circumferential compression by massive anthracotic calcified lymph nodes was noted in the surgical fields. A bypass graft was performed using an artificial vessel instead of endovascular treatment because of severe adhesion. The abrupt SVCS and uncontrolled pleural effusions completely disappeared after surgical correction.
Keywords: Superior vena cava syndrome (SVCS); mediastinal lymphadenopathy; pleural effusion.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

Similar articles
-
An unusual case of superior vena cava syndrome caused by the intravascular invasion of an invasive thymoma.Tuberc Respir Dis (Seoul). 2013 Nov;75(5):210-3. doi: 10.4046/trd.2013.75.5.210. Epub 2013 Nov 29. Tuberc Respir Dis (Seoul). 2013. PMID: 24348669 Free PMC article.
-
A Review of Open and Endovascular Treatment of Superior Vena Cava Syndrome of Benign Aetiology.Eur J Vasc Endovasc Surg. 2017 Feb;53(2):238-254. doi: 10.1016/j.ejvs.2016.11.013. Epub 2016 Dec 19. Eur J Vasc Endovasc Surg. 2017. PMID: 28007450 Review.
-
Superior vena cava syndrome caused by encapsulated pleural effusion.Eur Respir J. 1997 Jul;10(7):1675-7. doi: 10.1183/09031936.97.10071675. Eur Respir J. 1997. PMID: 9230264
-
Using Fenestrated Stent to Increase the Flow of Extracorporeal Membrane Oxygenation of Superior Vena Cava Compression Syndrome.Cureus. 2023 Sep 26;15(9):e46008. doi: 10.7759/cureus.46008. eCollection 2023 Sep. Cureus. 2023. PMID: 37766775 Free PMC article.
-
Malignant Superior Vena Cava Syndrome: State of the Art.Cureus. 2022 Jan 4;14(1):e20924. doi: 10.7759/cureus.20924. eCollection 2022 Jan. Cureus. 2022. PMID: 35004083 Free PMC article. Review.
References
-
- Parish JM, Marschke RF, Jr, Dines DE, et al. Etiologic considerations in superior vena cava syndrome. Mayo Clin Proc 1981;56:407-13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources