

The safety, efficacy, and treatment outcomes of a combination of low-dose decitabine treatment in patients with recurrent ovarian cancer
- PMID: 28932630
- PMCID: PMC5599090
- DOI: 10.1080/2162402X.2017.1323619
The safety, efficacy, and treatment outcomes of a combination of low-dose decitabine treatment in patients with recurrent ovarian cancer
Abstract
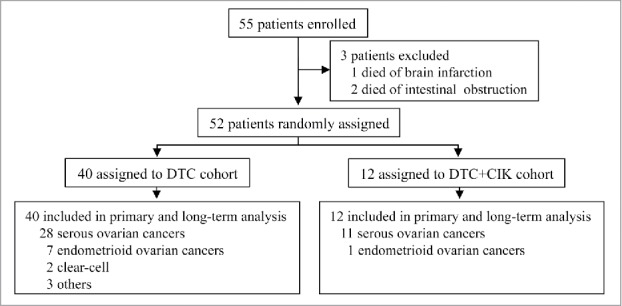
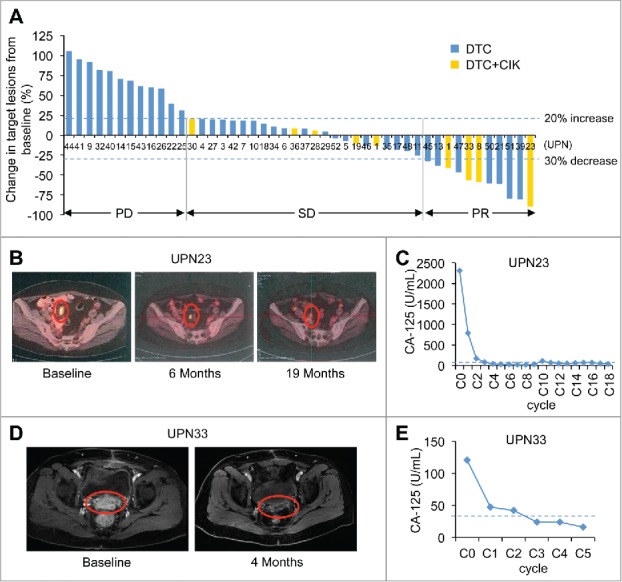
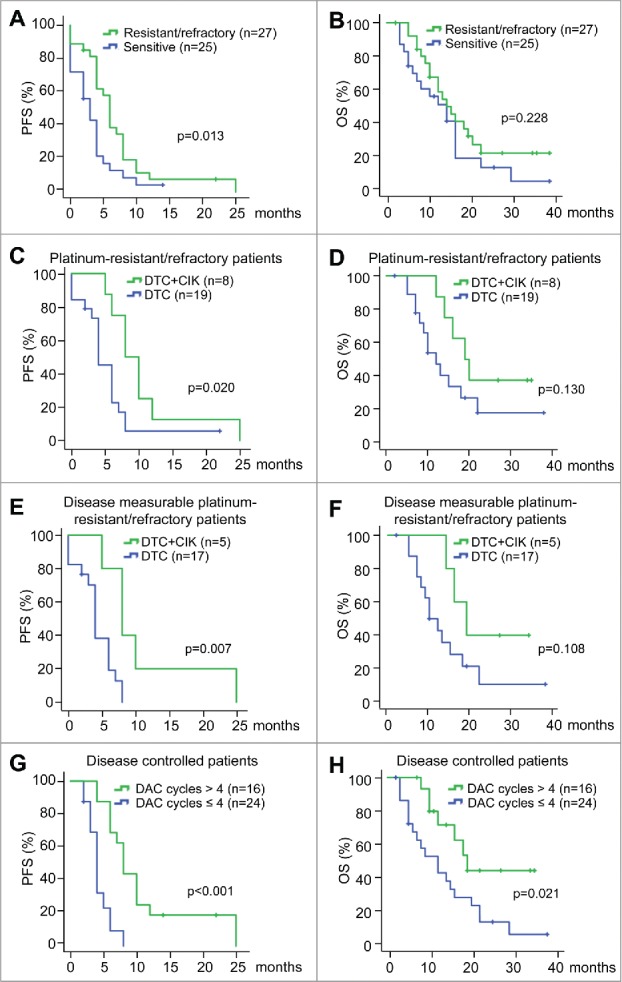
Purpose: DNA demethylating agents have shown clinical effectiveness in hematological and solid tumors. This trial tested the safety, efficacy, and treatment outcomes of decitabine-based chemotherapy or combined with immunotherapy in recurrent ovarian cancer patients. Patients and methods: Fifty-five patients with recurrent ovarian cancer were enrolled and 52 were assessable for clinical response and survival. Patients either received 5-d decitabine treatment, followed by reduced-dose of paclitaxel/carboplatin administration (DTC cohort), or the aforementioned regimen combined with cytokine-induced killer cells therapy (DTC+CIK cohort). The primary end point was clinical response rate and progression-free survival (PFS). Secondary evaluation included safety assessment and overall survival (OS). Results: Disease control rate (DCR) and objective response rate (ORR) were 73.91% and 23.91% in disease measurable patients by RECIST criteria, totally 76.92% and 30.77%, including disease non-measurable patients, which were higher in platinum-resistant/refractory patients. Clinical benefits could be associated with the number of DAC treatment cycles and the inclusion of CIK immunotherapy. In DTC+CIK cohort, DCR and ORR reached 100% and 58.30%, respectively. Notably, DTC+CIK treatment in platinum-resistant/refractory patients had an ORR of 87.50%. Consistently, PFS was longer in platinum-resistant/refractory patients comparing with that of platinum-sensitive patients. PFS and OS were 8 and 19 mo in platinum-resistant/refractory patients with DTC+CIK therapy. The most common toxicities were nausea, anorexia, fatigue, neutropenia, and anemia; many of which were grade 1-2. Conclusion: Low-dose DAC/paclitaxel/carboplatin regimen demonstrates disease benefit, especially in patients with platinum-resistant/refractory ovarian cancer, and might show remarkable clinical response when combined with adoptive immunotherapy in platinum-resistant/refractory ovarian cancer patients.
Keywords: CIK therapy; decitabine; epigenetic therapy; platinum sensitivity; recurrent ovarian cancer.
Figures
Similar articles
-
Phase Ib/II study of safety and efficacy of low-dose decitabine-primed chemoimmunotherapy in patients with drug-resistant relapsed/refractory alimentary tract cancer.Int J Cancer. 2018 Sep 15;143(6):1530-1540. doi: 10.1002/ijc.31531. Epub 2018 Apr 26. Int J Cancer. 2018. PMID: 29663379 Free PMC article. Clinical Trial.
-
Low Dose Decitabine Combined with Taxol and Platinum Chemotherapy to Treat Refractory/Recurrent Ovarian Cancer: An Open-Label, Single-Arm, Phase I/II Study.Curr Protein Pept Sci. 2015;16(4):329-36. doi: 10.2174/138920371604150429155740. Curr Protein Pept Sci. 2015. PMID: 25929868 Clinical Trial.
-
Phase IB Dose Escalation and Expansion Study of AKT Inhibitor Afuresertib with Carboplatin and Paclitaxel in Recurrent Platinum-resistant Ovarian Cancer.Clin Cancer Res. 2019 Mar 1;25(5):1472-1478. doi: 10.1158/1078-0432.CCR-18-2277. Epub 2018 Dec 18. Clin Cancer Res. 2019. PMID: 30563934 Clinical Trial.
-
Dose-dense chemotherapy with weekly paclitaxel and 3-weekly carboplatin for recurrent ovarian cancer.Taiwan J Obstet Gynecol. 2020 Jan;59(1):21-27. doi: 10.1016/j.tjog.2019.10.003. Taiwan J Obstet Gynecol. 2020. PMID: 32039795 Review.
-
Efficacy and safety of dendritic cells co-cultured with cytokine-induced killer cells immunotherapy for non-small-cell lung cancer.Int Immunopharmacol. 2015 Sep;28(1):22-8. doi: 10.1016/j.intimp.2015.05.021. Epub 2015 May 23. Int Immunopharmacol. 2015. PMID: 26013109 Review.
Cited by
-
DNA methylation in human diseases.Heliyon. 2024 Jun 4;10(11):e32366. doi: 10.1016/j.heliyon.2024.e32366. eCollection 2024 Jun 15. Heliyon. 2024. PMID: 38933971 Free PMC article. Review.
-
Everolimus combined with 5-aza-2-deoxycytidine generated potent anti-tumor effects on ovarian clear cell cancer stem-like/spheroid cells by inhibiting the COL6A3-AKT-mTOR pathway.Am J Cancer Res. 2022 Apr 15;12(4):1686-1706. eCollection 2022. Am J Cancer Res. 2022. PMID: 35530273 Free PMC article.
-
Chemotherapeutic and targeted drugs-induced immunogenic cell death in cancer models and antitumor therapy: An update review.Front Pharmacol. 2023 Apr 21;14:1152934. doi: 10.3389/fphar.2023.1152934. eCollection 2023. Front Pharmacol. 2023. PMID: 37153795 Free PMC article. Review.
-
LAMA3 DNA methylation and transcriptome changes associated with chemotherapy resistance in ovarian cancer.J Ovarian Res. 2021 May 15;14(1):67. doi: 10.1186/s13048-021-00807-y. J Ovarian Res. 2021. PMID: 33992120 Free PMC article.
-
Decitabine induces IRF7-mediated immune responses in p53-mutated triple-negative breast cancer: a clinical and translational study.Front Med. 2024 Apr;18(2):357-374. doi: 10.1007/s11684-023-1016-8. Epub 2023 Dec 29. Front Med. 2024. PMID: 38157193
References
-
- Thigpen JT, Blessing JA, Ball H, Hummel SJ, Barrett RJ. Phase II trial of paclitaxel in patients with progressive ovarian carcinoma after platinum-based chemotherapy: A gynecologic oncology group study. J Clin Oncol 1994; 12:1748-53; PMID:7916038; https://doi.org/10.1200/JCO.1994.12.9.1748 - DOI - PubMed
-
- Pujade-Lauraine E. How to approach patients in relapse. Ann Oncol 2012; 23(Suppl 10):x128-31; PMID:22987947; https://doi.org/10.1093/annonc/mds358 - DOI - PubMed
-
- Markman M, Rothman R, Hakes T, Reichman B, Hoskins W, Rubin S, Jones W, Almadrones L, Lewis JL Jr. Second-line platinum therapy in patients with ovarian cancer previously treated with cisplatin. J Clin Oncol 1991; 9:389-93; PMID:1999708; https://doi.org/10.1200/JCO.1991.9.3.389 - DOI - PubMed
-
- Cannistra SA. Is there a “best” choice of second-line agent in the treatment of recurrent, potentially platinum-sensitive ovarian cancer? J Clin Oncol 2002; 20:1158-60; PMID:11870154; https://doi.org/10.1200/JCO.2002.20.5.1158 - DOI - PubMed
-
- Vaughan S, Coward JI, Bast RC Jr., Berchuck A, Berek JS, Brenton JD, Coukos G, Crum CC, Drapkin R, Etemadmoghadam D et al.. Rethinking ovarian cancer: Recommendations for improving outcomes. Nat Rev Cancer 2011; 11:719-25; PMID:21941283; https://doi.org/10.1038/nrc3144 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources