

Thoracic wall trauma-misdiagnosed lesions on radiographs and usefulness of ultrasound, multidetector computed tomography and magnetic resonance imaging
- PMID: 28932697
- PMCID: PMC5594019
- DOI: 10.21037/qims.2017.08.02
Thoracic wall trauma-misdiagnosed lesions on radiographs and usefulness of ultrasound, multidetector computed tomography and magnetic resonance imaging
Abstract
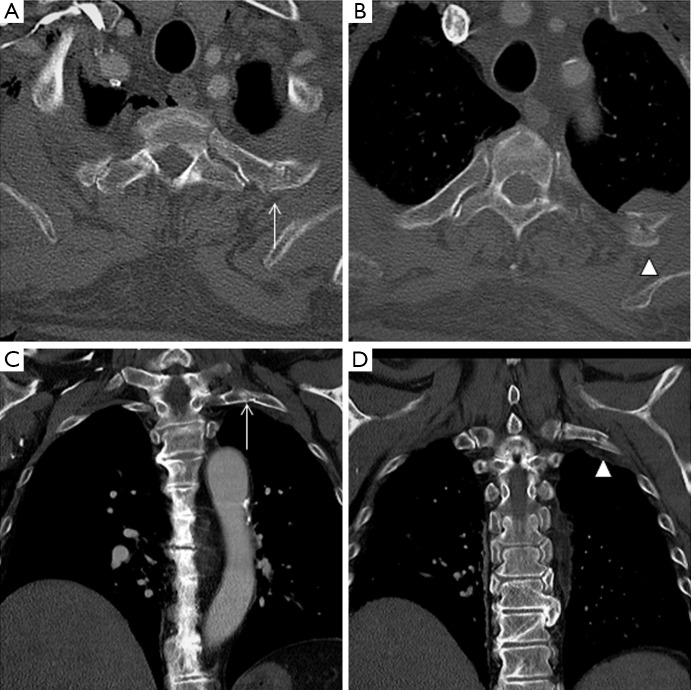
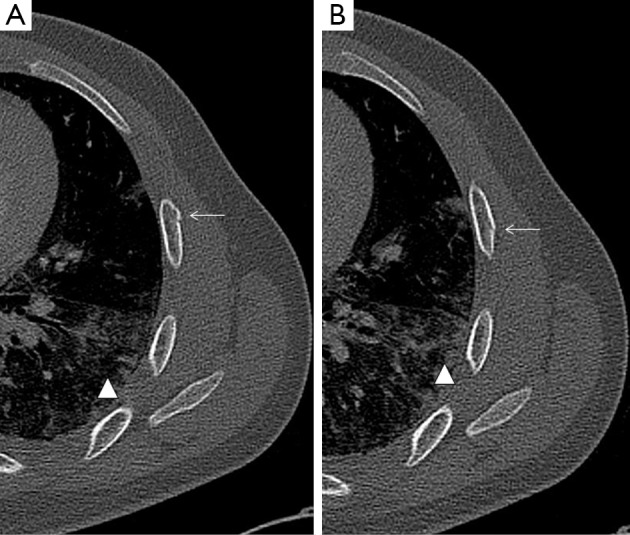
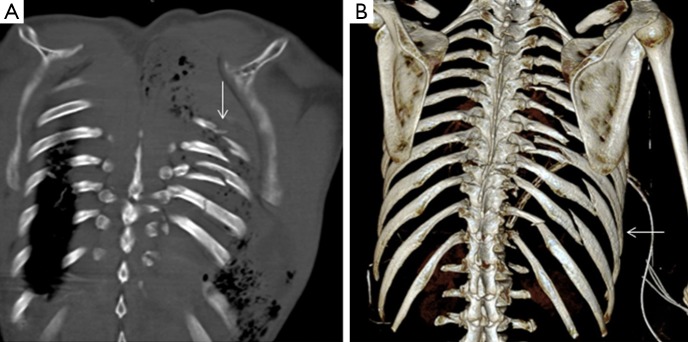
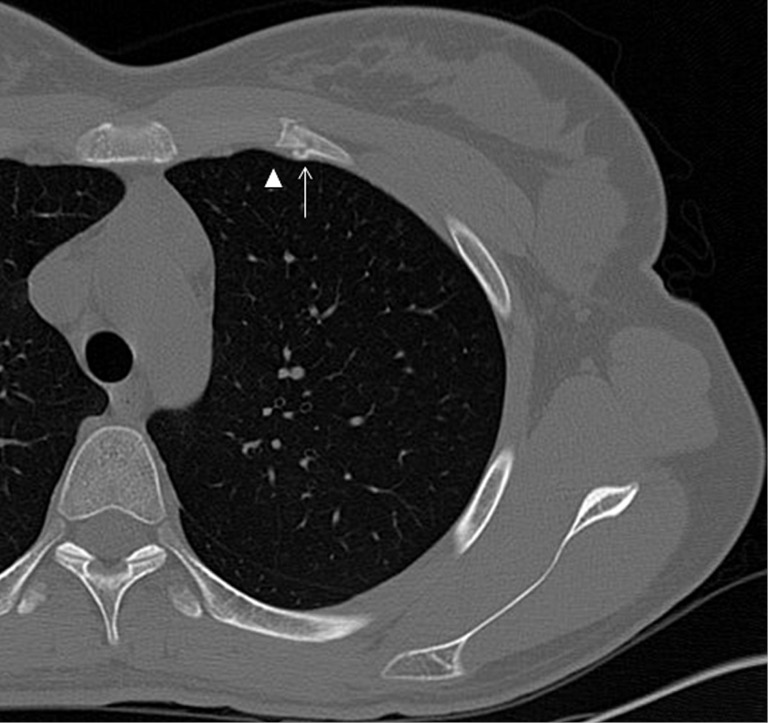
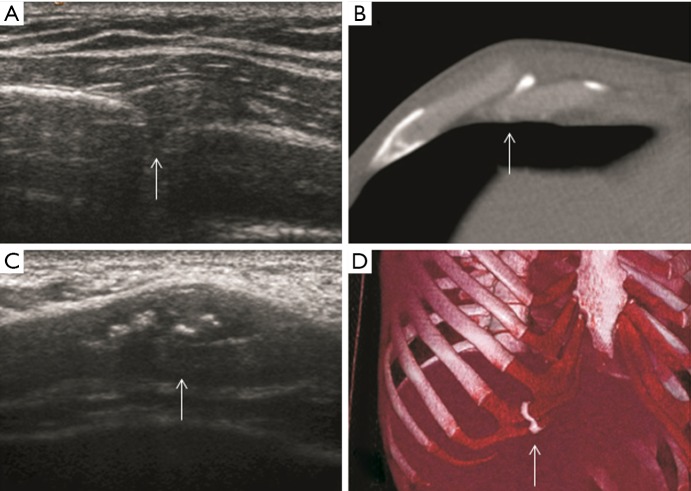
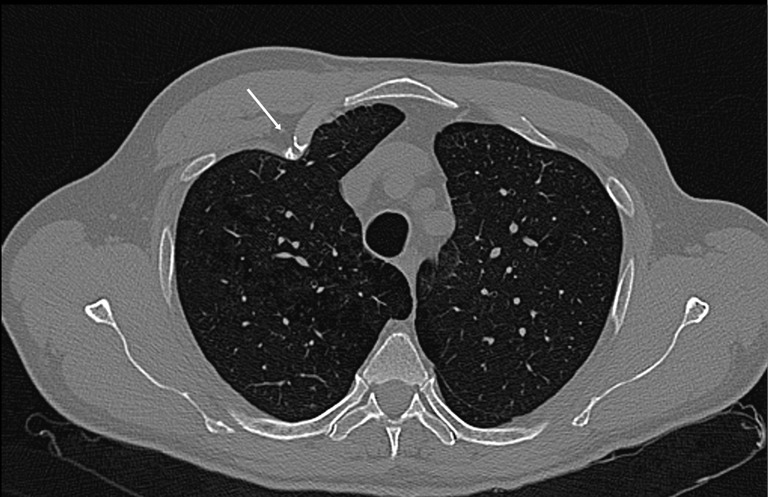
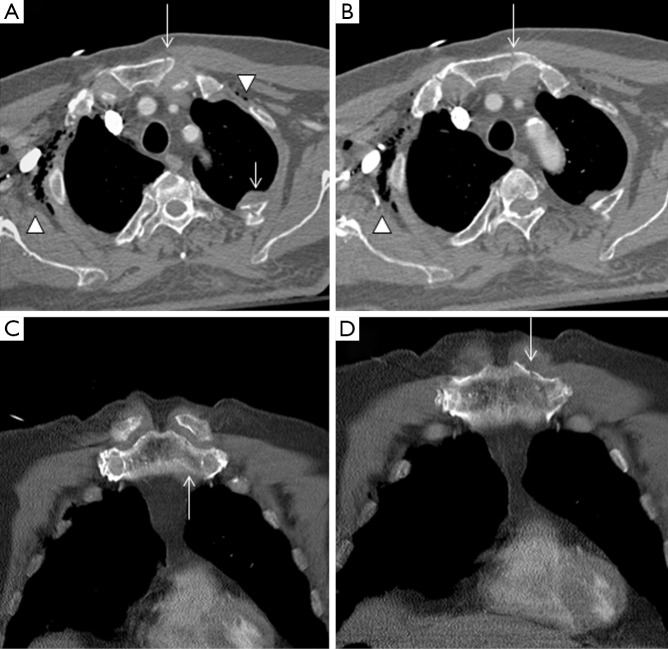
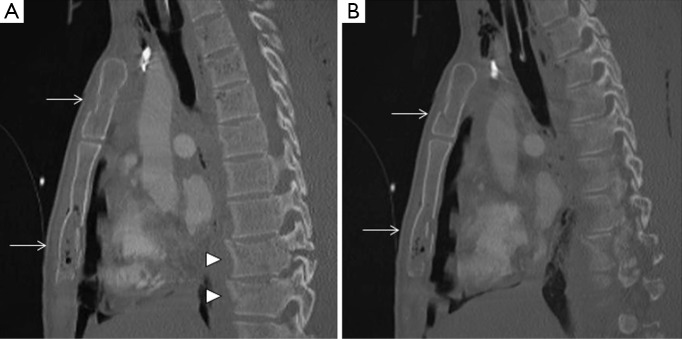
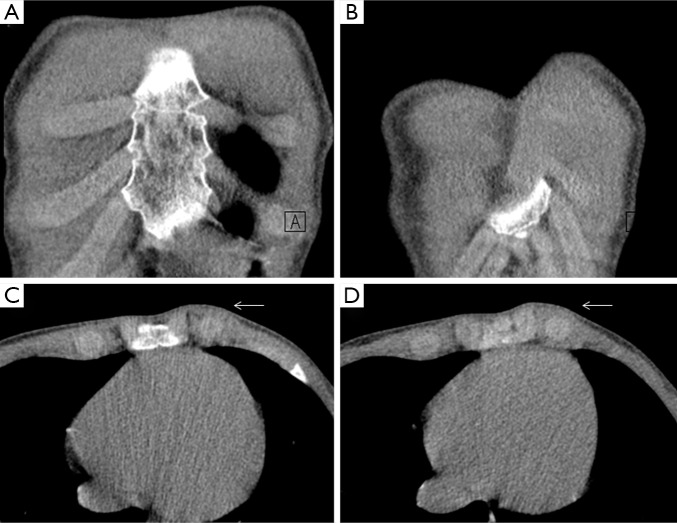
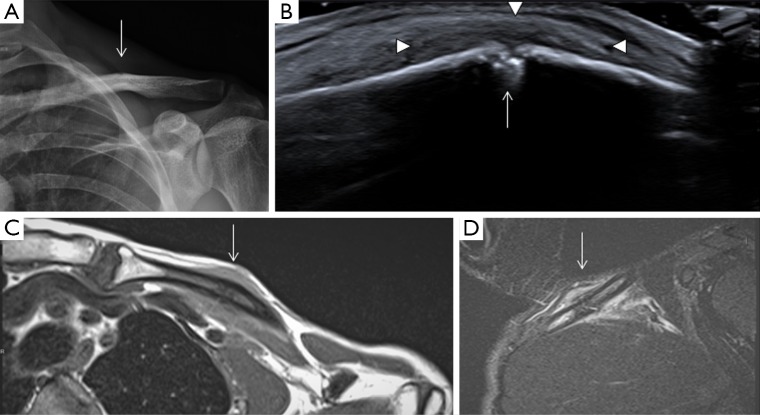
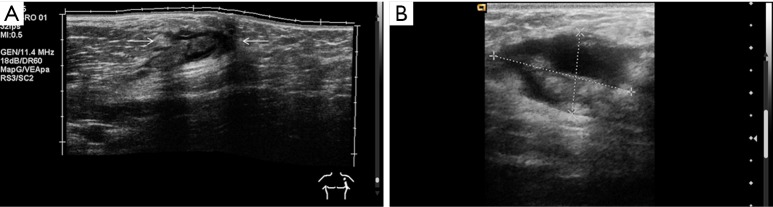
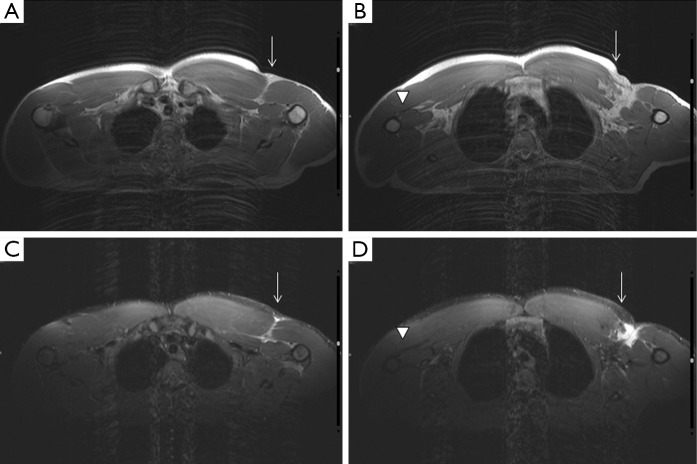
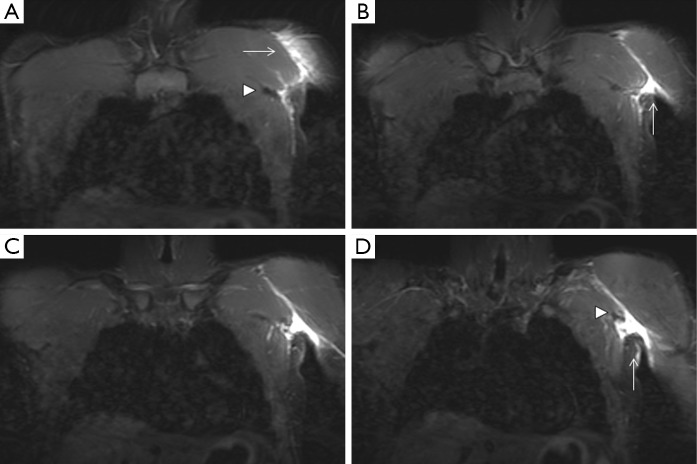
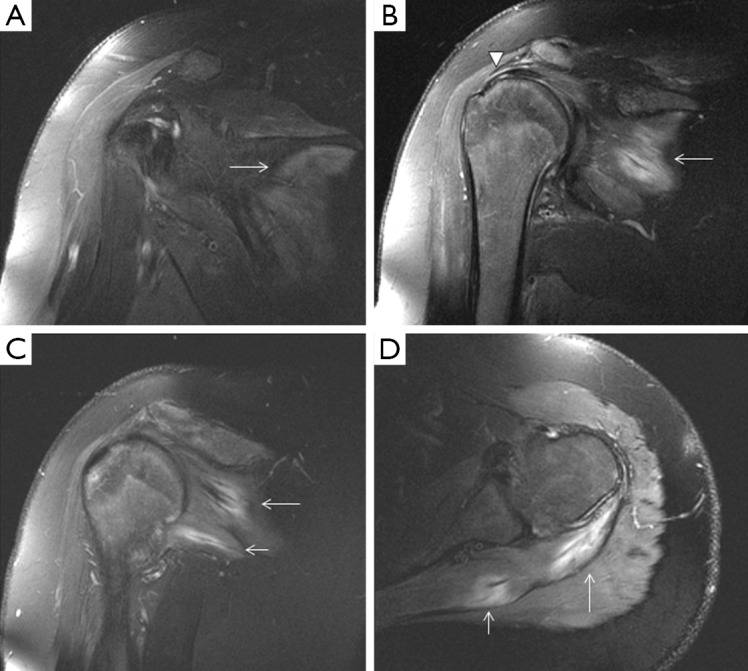
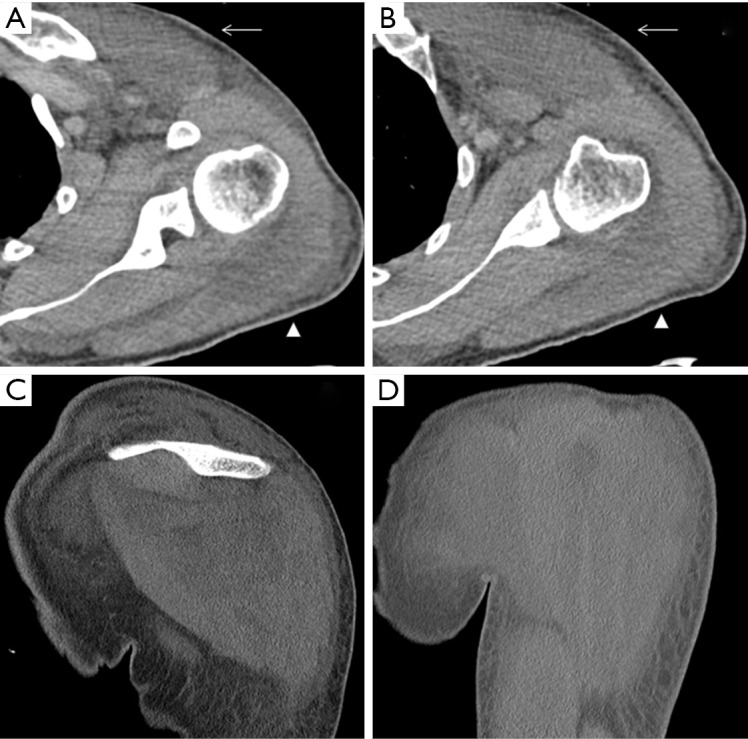
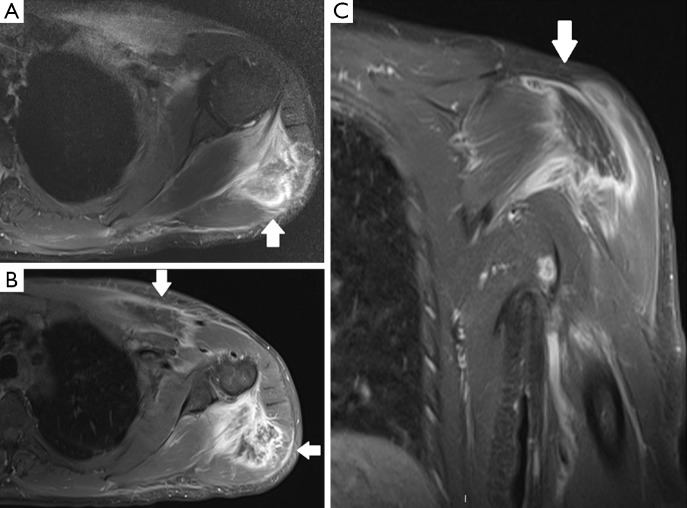
Blunt injuries to the chest wall are an important chapter on emergency room (ER) departments, being the third most common injuries in trauma patients which ominous complications could appear. This article describes different types of traumatic events affecting the chest wall, which maybe misdiagnosed with conventional X-ray. Special emphasis has been done in computed tomography (CT) and multidetector CT (MDCT) imaging. This technique is considered the "gold-standard" for those traumatic patients, due to its fast acquisition covering the whole area of interest in axial plane, reconstructing multiplanar (2D, 3D) volume-rendered images with a superb quality and angiographic CT capabilities for evaluating vascular damage. Complementary techniques such as ultrasonography (US) and magnetic resonance imaging (MRI) may improve the diagnostic accuracy due to its great capacity in visualising soft-tissue trauma (muscle-tendinous tears) and subtle fractures. All these imaging methods have an important role in quantifying the severity of chest wall trauma. The findings of this study have been exposed with cases of our archives in a didactic way.
Keywords: Magnetic resonance imaging (MRI); injuries; multidetector computed tomography (MDCT); thoracic wall; ultrasonography (US); wounds.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- The American College of Surgeons Committee on Trauma Leadership. In: Clark DE, Fantus RJ, eds. National Trauma Data Bank (NTDB) Annual Report 2007. Chicago: American College of Surgeons, 2007:1-64.
-
- Omert L, Yeaney WW, Protetch J. Efficacy of thoracic computerized tomography in blunt chest trauma. Am Surg 2001;67:660-4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources