

Imaging in traumatic mandibular fractures
- PMID: 28932703
- PMCID: PMC5594017
- DOI: 10.21037/qims.2017.08.06
Imaging in traumatic mandibular fractures
Abstract
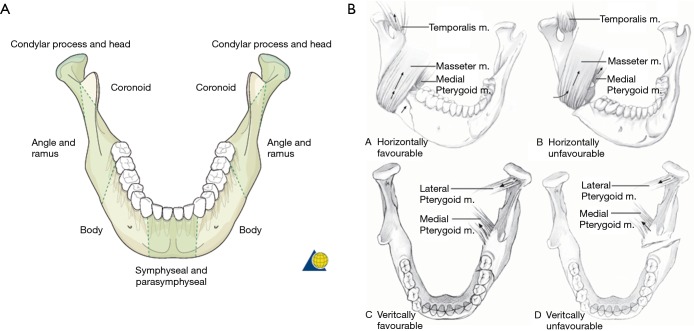
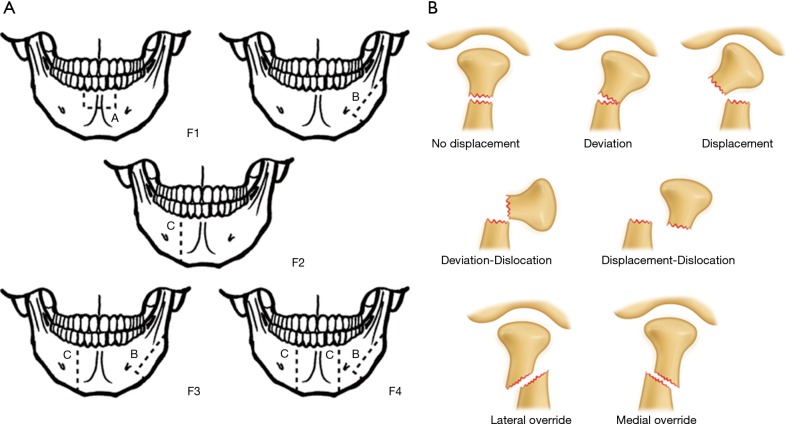
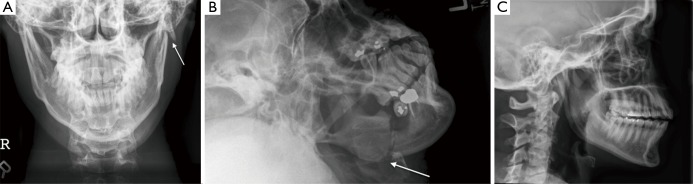
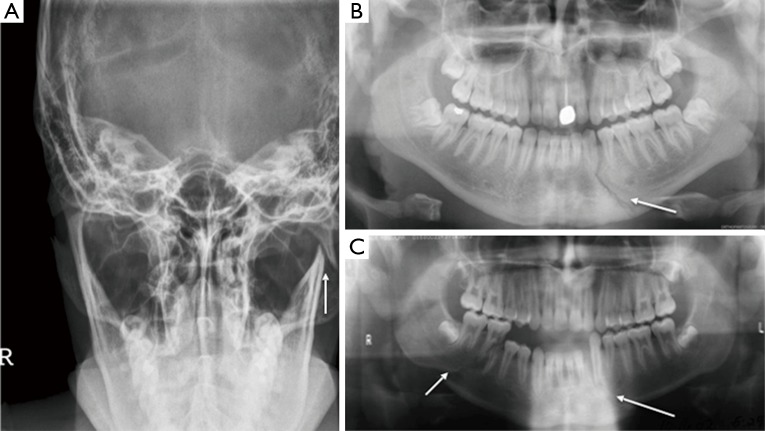
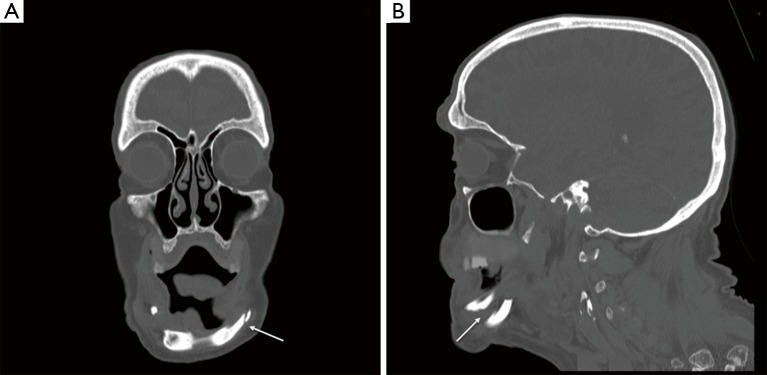
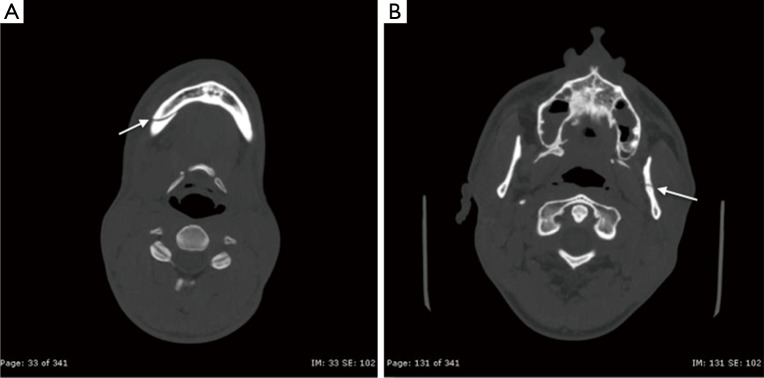
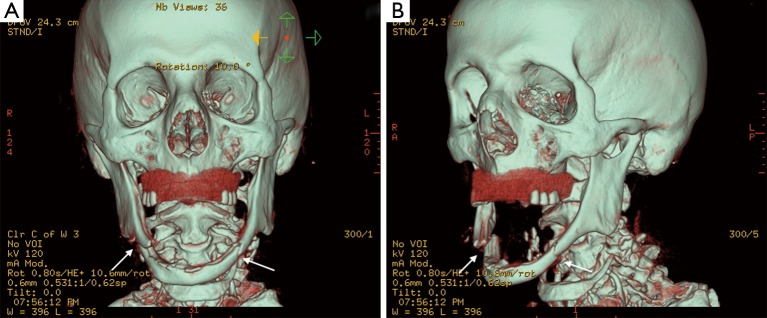
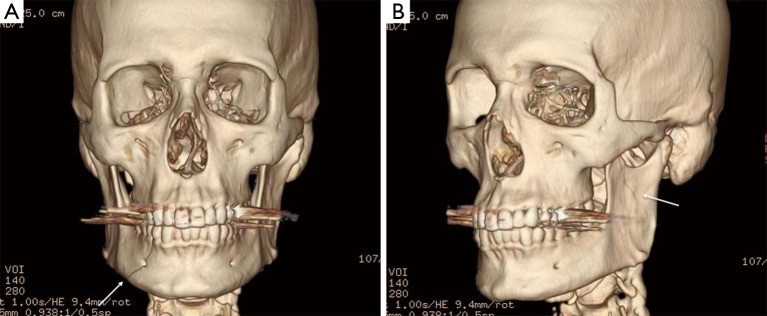
A fracture of the mandible is a common trauma presentation amongst young males and represents one of the most frequently encountered fractured bones within the viscerocranium. Historically, assault was the dominant contributing factor but now due to the increased number of vehicles used per capita, motor vehicle accidents are the primary cause. Mandibular fractures can be classified anatomically, by dentition, by muscle group and by severity. The fracture may also be closed, open, comminuted, displaced or pathological. It is important that the imaging modality used identifies the classification as this will decide definitive treatment. X-ray projections have typically been used to detect a mandibular fracture, but are limited to an anteroposterior (AP), lateral and oblique view in an unstable trauma patient. These views are inadequate to detail the level of fracture displacement and show poor detail of the condylar region. Computer tomography (CT) is the imaging modality of choice when assessing a traumatic mandibular injury and can demonstrate a 100% sensitivity in detecting a fracture. This is through use of a multidetector-row CT, which reduces motion blur and therefore produces accurate coronal and sagittal reconstructions. Furthermore, reconstructive three-dimensional CT images gained from planar views, allows a better understanding of the spatial relationship of the fracture with other anatomical landmarks. This ensures a better appreciation of the severity and classification of a mandibular fracture, which therefore influences operative planning. Ultrasound is another useful modality in detecting a mandibular fracture when the patient is too unstable to be transferred to a CT scanner. The sensitivity however is less in comparison to a CT series of images and provides limited detail on the fracture pattern. Magnetic resonance imaging demonstrates use in assessing soft tissue injury of the temporomandibular joint but this is unlikely to be of priority when initially assessing a trauma patient.
Keywords: 3D reconstruction; Mandibular fracture; X-ray vs. CT; classification of fractures; trauma; trauma imaging.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Role of Multidetector Computed Tomography in the Evaluation of Maxillofacial Trauma.Cureus. 2023 Feb 15;15(2):e35008. doi: 10.7759/cureus.35008. eCollection 2023 Feb. Cureus. 2023. PMID: 36938234 Free PMC article.
-
Radiological investigation of acute mandibular injury.Natl J Maxillofac Surg. 2022 May-Aug;13(2):165-171. doi: 10.4103/njms.NJMS_27_19. Epub 2022 Jul 15. Natl J Maxillofac Surg. 2022. PMID: 36051802 Free PMC article. Review.
-
Vertically unstable fractured mandibular segment with attached genial tubercles as a parameter for difficulty during intubation for general anaesthesia-substantiation with computed tomographic (CT) scan evidence.Oral Maxillofac Surg. 2019 Jun;23(2):215-219. doi: 10.1007/s10006-019-00768-z. Epub 2019 May 9. Oral Maxillofac Surg. 2019. PMID: 31073651
-
Intracapsular condylar fracture of the mandible: our classification and open treatment experience.J Oral Maxillofac Surg. 2009 Aug;67(8):1672-9. doi: 10.1016/j.joms.2009.02.012. J Oral Maxillofac Surg. 2009. PMID: 19615581
-
Imaging of Scaphoid Fractures According to the New S3 Guidelines.Rofo. 2016 May;188(5):459-69. doi: 10.1055/s-0042-104660. Epub 2016 Apr 13. Rofo. 2016. PMID: 27074424 Review. English.
Cited by
-
Imaging of traumatic mandibular fractures in young adults using CT-like MRI: a feasibility study.Clin Oral Investig. 2023 Mar;27(3):1227-1233. doi: 10.1007/s00784-022-04736-y. Epub 2022 Oct 8. Clin Oral Investig. 2023. PMID: 36208329 Free PMC article.
-
Traumatic genial tubercle fracture: a case description with 9-month radiographic follow-up and a literature analysis.Quant Imaging Med Surg. 2022 Apr;12(4):2579-2585. doi: 10.21037/qims-21-736. Quant Imaging Med Surg. 2022. PMID: 35371931 Free PMC article. No abstract available.
-
Conservative management of mandibular fractures in pediatric patients during the growing phase with splint fiber and ligature arch wire.BMC Oral Health. 2023 Aug 28;23(1):601. doi: 10.1186/s12903-023-03309-z. BMC Oral Health. 2023. PMID: 37641075 Free PMC article.
-
Diagnosis of split fractures of the mandible in adults.Arch Craniofac Surg. 2023 Aug;24(4):167-173. doi: 10.7181/acfs.2023.00290. Epub 2023 Aug 20. Arch Craniofac Surg. 2023. PMID: 37654236 Free PMC article.
-
Functional Rehabilitation after Mandibular Fracture - A Systematic Review.Ann Maxillofac Surg. 2022 Jul-Dec;12(2):197-202. doi: 10.4103/ams.ams_99_22. Epub 2023 Jan 10. Ann Maxillofac Surg. 2022. PMID: 36874767 Free PMC article. Review.
References
-
- Laub DR. Mandibular Fractures. Medscape. 2016 Jan 14. Available online: http://emedicine.medscape.com/article/1283150-overview#a4
-
- Soule WC, Fisher LH. Mandibular Fracture Imaging. Medscape. 2015 Jul 01. Available online: http://emedicine.medscape.com/article/391549-overview
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources