

Comparison of morbidity-related seroma formation following conventional latissimus dorsi flap versus muscle-sparing latissimus dorsi flap breast reconstruction
- PMID: 28932726
- PMCID: PMC5597534
- DOI: 10.4174/astr.2017.93.3.119
Comparison of morbidity-related seroma formation following conventional latissimus dorsi flap versus muscle-sparing latissimus dorsi flap breast reconstruction
Abstract
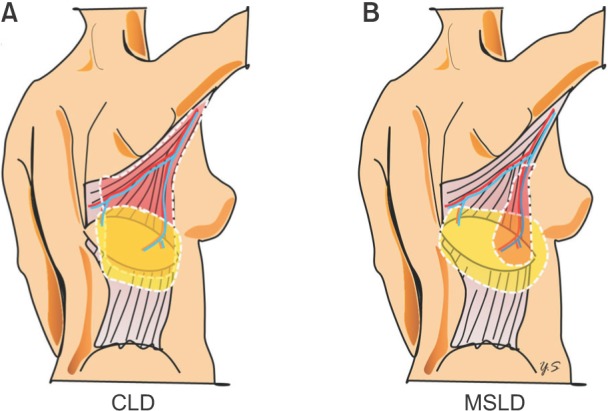
Purpose: The pedicled, descending-branch muscle-sparing latissimus dorsi (MSLD) flap has been widely used for breast reconstruction following total mastectomy. However, the superiority of the MSLD flap compared to the conventional latissimus dorsi (CLD) flap in preventing seroma formation has not been demonstrated. This study compares the morbidities related to seroma formation following pedicled MSLD flap and CLD flap breast reconstruction.
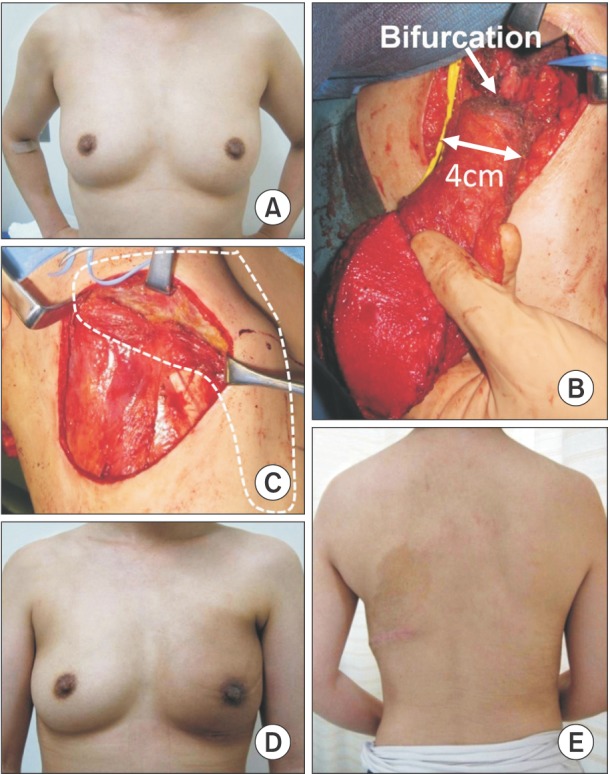
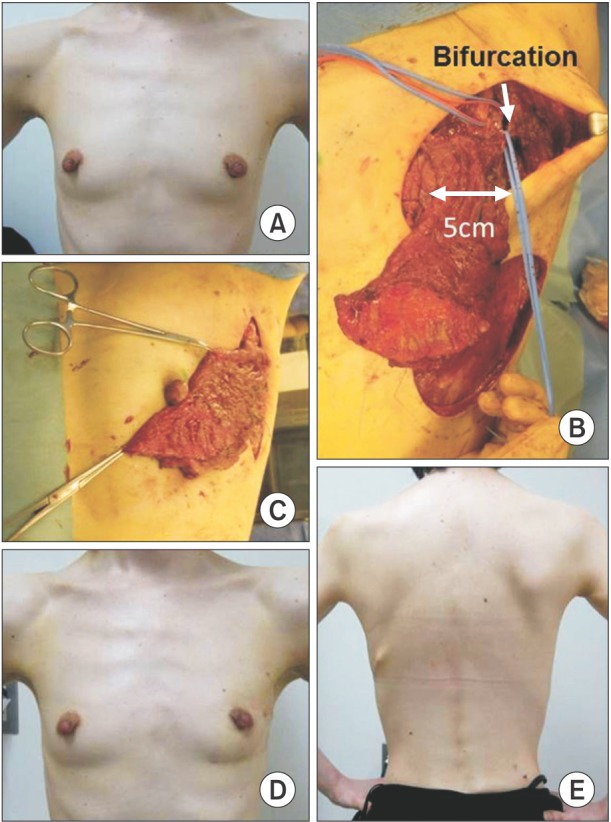
Methods: A total of 15 women who underwent partial mastectomy and immediate partial breast reconstruction with MSLD flaps were compared with 15 women under identical conditions with CLD flap breast reconstruction. The medical records were reviewed for both complications and demographic data. The authors compared morbidity, including donor-site seroma, total volume of drain discharge, indwelling period of drainage, and length of hospital stay following both MSLD flap and CLD flap breast reconstruction.
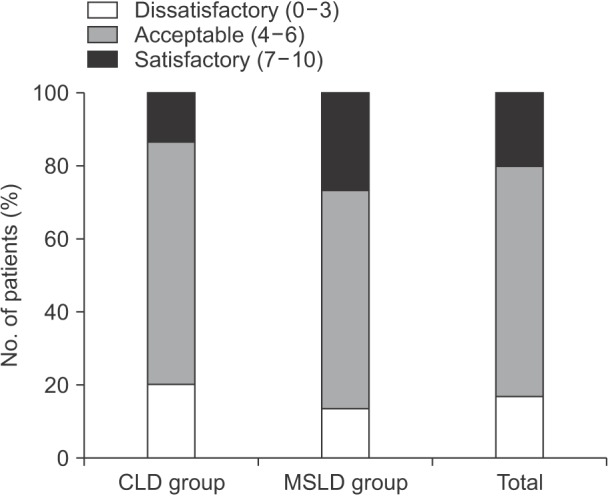
Results: The demographic data of the 2 groups were not significantly different. Donor-site seroma occurred in 2 MSLD patients (13.3%) and in 6 CLD patients (40.0%). The total volume of the drain discharge and the indwelling period of drainage at donor site were significantly lower in the MSLD group. The length of hospital stay was significantly shorter (by approximately a day and a half) for the MSLD group.
Conclusion: The MSLD flap, with its low complication rate and associated minimal functional and aesthetic deficits at the donor site, may be a useful option for small breast reconstruction if earlier discharge from hospital is demanded.
Keywords: Mammaplasty; Seroma; Superficial back muscles.
Conflict of interest statement
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Evaluation of seromas in postmastectomy breast reconstruction: A retrospective observational study.JPRAS Open. 2021 Nov 24;31:105-113. doi: 10.1016/j.jpra.2021.11.001. eCollection 2022 Mar. JPRAS Open. 2021. PMID: 34988276 Free PMC article.
-
Comparison of morbidity of donor site following pedicled muscle-sparing latissimus dorsi flap versus extended latissimus dorsi flap breast reconstruction.J Plast Reconstr Aesthet Surg. 2013 May;66(5):640-6. doi: 10.1016/j.bjps.2013.01.026. Epub 2013 Feb 18. J Plast Reconstr Aesthet Surg. 2013. PMID: 23428931
-
Comparison of postoperative complications following conventional latissimus dorsi flap versus muscle-sparing latissimus dorsi flap breast reconstruction.J Plast Reconstr Aesthet Surg. 2022 Oct;75(10):3653-3663. doi: 10.1016/j.bjps.2022.06.084. Epub 2022 Jul 23. J Plast Reconstr Aesthet Surg. 2022. PMID: 36100540 Review.
-
Comparison of post-operative complications after immediate breast reconstruction by muscle-sparing latissimus dorsi flap versus total latissimus dorsi flap.Bull Cancer. 2025 Jul-Aug;112(7-8):893-903. doi: 10.1016/j.bulcan.2025.02.027. Epub 2025 Jun 16. Bull Cancer. 2025. PMID: 40527719
-
[Sequelae after harvesting latissimus dorsi flap and derivates--review].Ann Chir Plast Esthet. 2014 Oct;59(5):348-54. doi: 10.1016/j.anplas.2014.05.002. Epub 2014 Jun 16. Ann Chir Plast Esthet. 2014. PMID: 24947671 Review. French.
Cited by
-
Evaluation of seromas in postmastectomy breast reconstruction: A retrospective observational study.JPRAS Open. 2021 Nov 24;31:105-113. doi: 10.1016/j.jpra.2021.11.001. eCollection 2022 Mar. JPRAS Open. 2021. PMID: 34988276 Free PMC article.
-
Oncoplastic Volume Replacement for Breast Cancer: Latissimus Dorsi Flap versus Thoracodorsal Artery Perforator Flap.Plast Reconstr Surg Glob Open. 2019 Oct 30;7(10):e2476. doi: 10.1097/GOX.0000000000002476. eCollection 2019 Oct. Plast Reconstr Surg Glob Open. 2019. PMID: 31772899 Free PMC article.
-
Preventive Effect on Seroma of Use of PEAK PlasmaBlade after Latissimus Dorsi Breast Reconstruction.Plast Reconstr Surg Glob Open. 2018 Dec 17;6(12):e2035. doi: 10.1097/GOX.0000000000002035. eCollection 2018 Dec. Plast Reconstr Surg Glob Open. 2018. PMID: 30656116 Free PMC article.
-
Cubital fossa defect- our reconstructive experience with pedicle flaps.J Orthop. 2022 Apr 30;32:7-12. doi: 10.1016/j.jor.2022.04.013. eCollection 2022 Jul-Aug. J Orthop. 2022. PMID: 35585945 Free PMC article.
-
Conversion of Breast Implants into Natural Breast Reconstruction: Evaluating Lipofilled Mini Dorsi Flap.Plast Reconstr Surg Glob Open. 2022 Jul 25;10(7):e4450. doi: 10.1097/GOX.0000000000004450. eCollection 2022 Jul. Plast Reconstr Surg Glob Open. 2022. PMID: 35923995 Free PMC article.
References
-
- Clough KB, Louis-Sylvestre C, Fitoussi A, Couturaud B, Nos C. Donor site sequelae after autologous breast reconstruction with an extended latissimus dorsi flap. Plast Reconstr Surg. 2002;109:1904–1911. - PubMed
-
- Roy MK, Shrotia S, Holcombe C, Webster DJ, Hughes LE, Mansel RE. Complications of latissimus dorsi myocutaneous flap breast reconstruction. Eur J Surg Oncol. 1998;24:162–165. - PubMed
-
- Schwabegger A, Ninkovic M, Brenner E, Anderl H. Seroma as a common donor site morbidity after harvesting the latissimus dorsi flap: observations on cause and prevention. Ann Plast Surg. 1997;38:594–597. - PubMed
-
- Saint-Cyr M, Nagarkar P, Schaverien M, Dauwe P, Wong C, Rohrich RJ. The pedicled descending branch muscle-sparing latissimus dorsi flap for breast reconstruction. Plast Reconstr Surg. 2009;123:13–24. - PubMed
-
- Brackley PT, Mishra A, Sigaroudina M, Iqbal A. Modified muscle sparing latissimus dorsi with implant for total breast reconstruction - extending the boundaries. J Plast Reconstr Aesthet Surg. 2010;63:1495–1502. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
