

Comparative effectiveness of different transarterial embolization therapies alone or in combination with local ablative or adjuvant systemic treatments for unresectable hepatocellular carcinoma: A network meta-analysis of randomized controlled trials
- PMID: 28934265
- PMCID: PMC5608206
- DOI: 10.1371/journal.pone.0184597
Comparative effectiveness of different transarterial embolization therapies alone or in combination with local ablative or adjuvant systemic treatments for unresectable hepatocellular carcinoma: A network meta-analysis of randomized controlled trials
Abstract
Background: The optimal transcatheter embolization strategy for patients with unresectable hepatocellular carcinoma (HCC) remains elusive. We conducted a systematic review and network meta-analysis (NMA) of different embolization options for unresectable HCC.
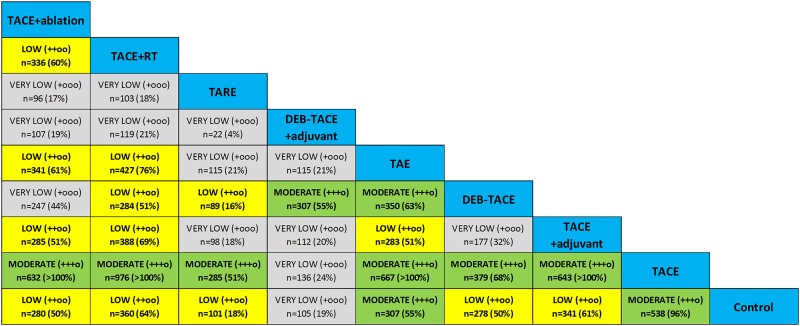
Methods: Medical databases were searched for randomized controlled trials evaluating bland transarterial embolization (TAE), conventional TACE, drug-eluting bead chemoembolization (DEB-TACE), or transarterial radioembolization (TARE), either alone or combined with adjuvant chemotherapy, or local liver ablation, or external radiotherapy for unresectable HCC up to June 2017. Random effects Bayesian models with a binomial and normal likelihood were fitted (WinBUGS). Primary endpoint was patient survival expressed as hazard ratios (HR) and 95% credible intervals. An exponential model was used to fit patient survival curves. Safety and objective response were calculated as odds ratios (OR) and accompanying 95% credible intervals. Competing treatments were ranked with the SUCRA statistic. Heterogeneity-adjusted effective sample sizes were calculated to evaluate information size for each comparison. Quality of evidence (QoE) was assessed with the GRADE system adapted for NMA reports. All analyses complied with the ISPOR-AMCP-NCP Task Force Report for good practice in NMA.
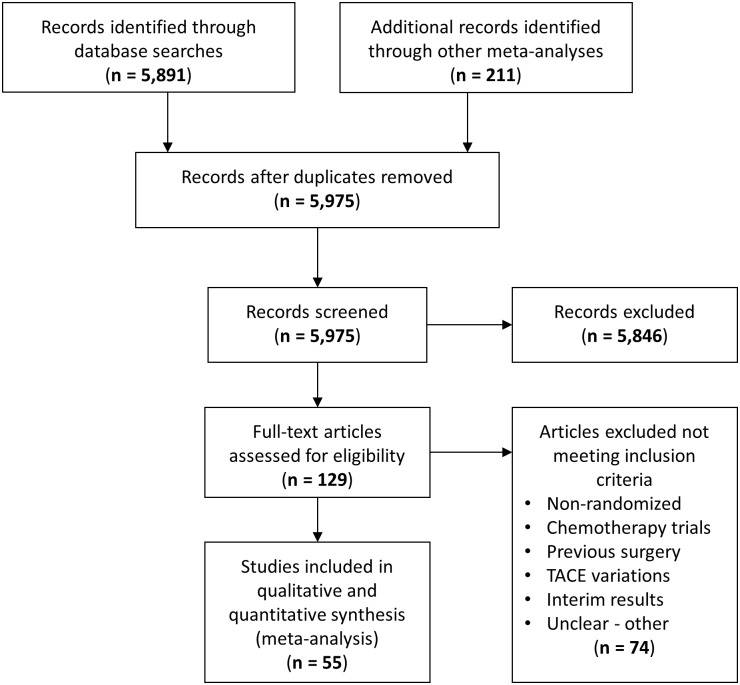
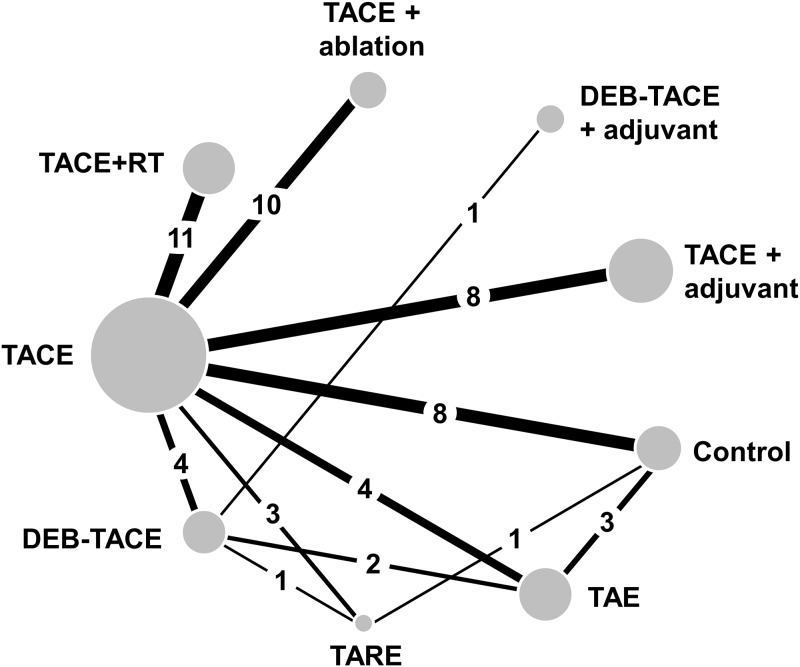
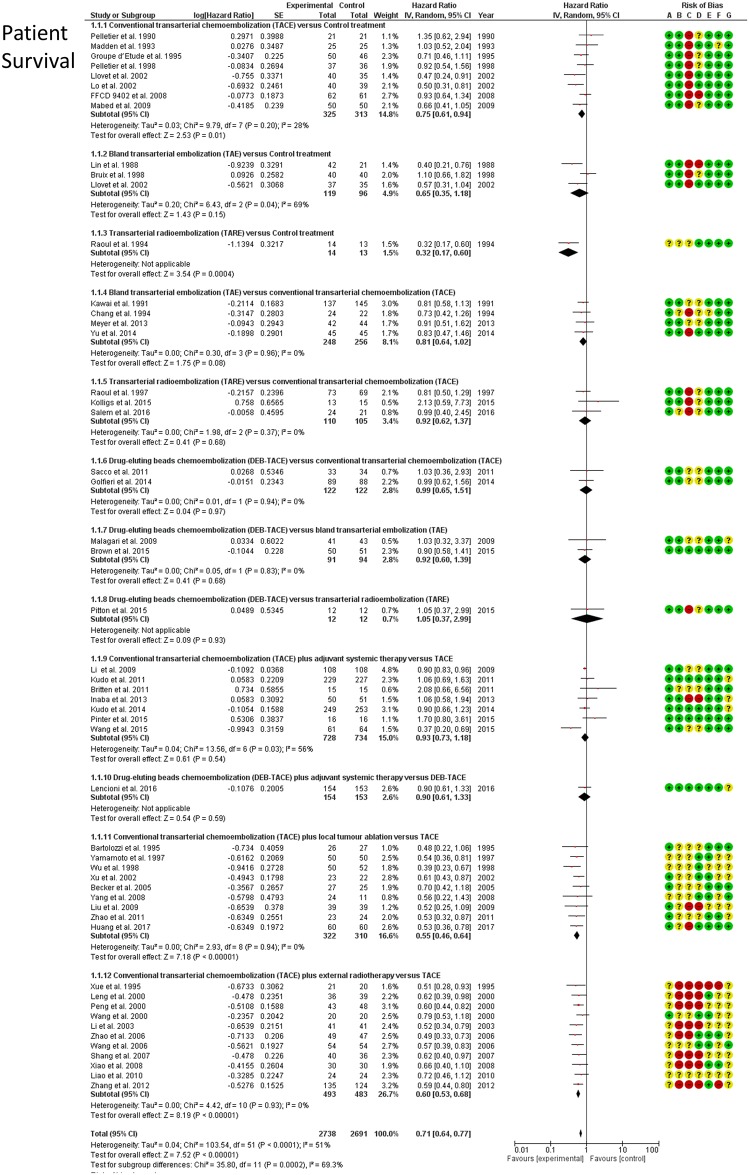
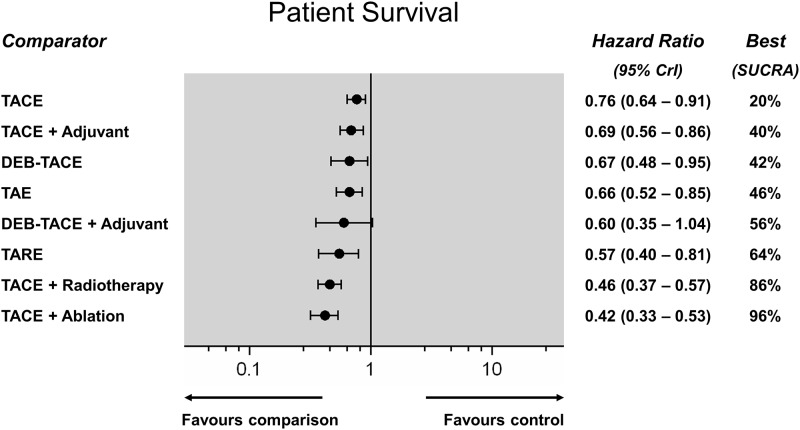
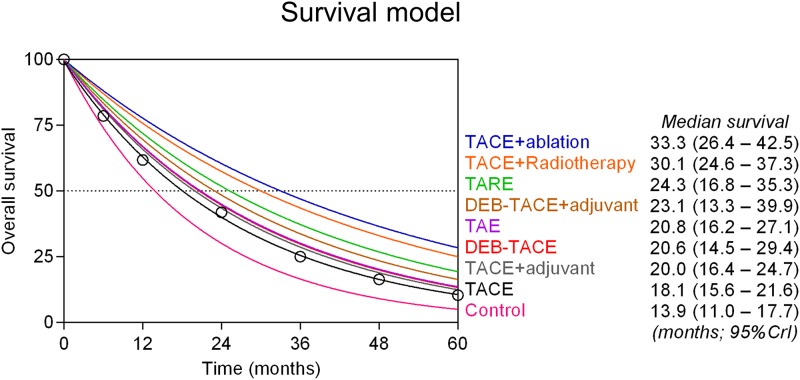
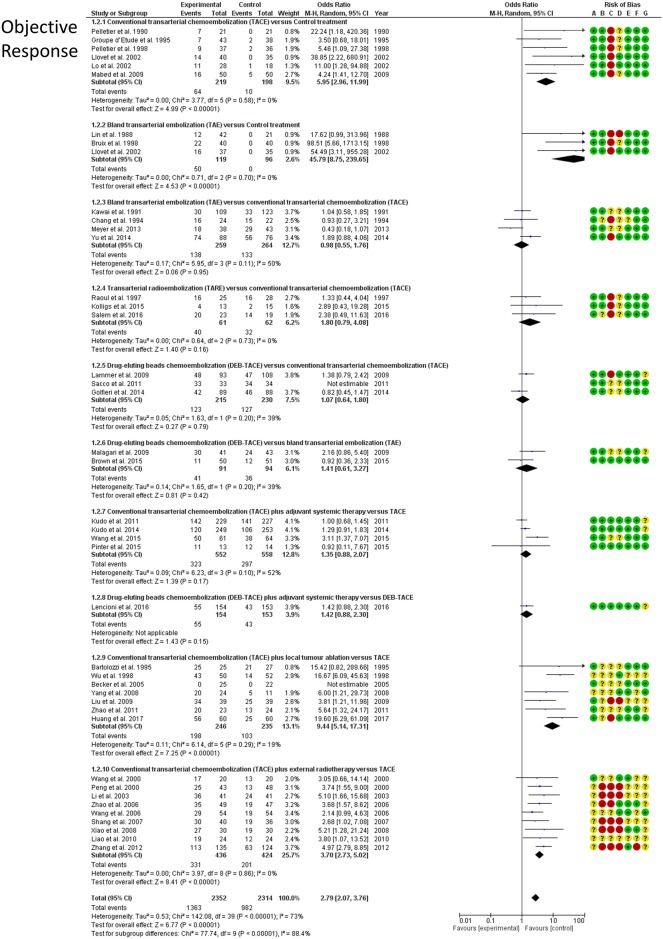
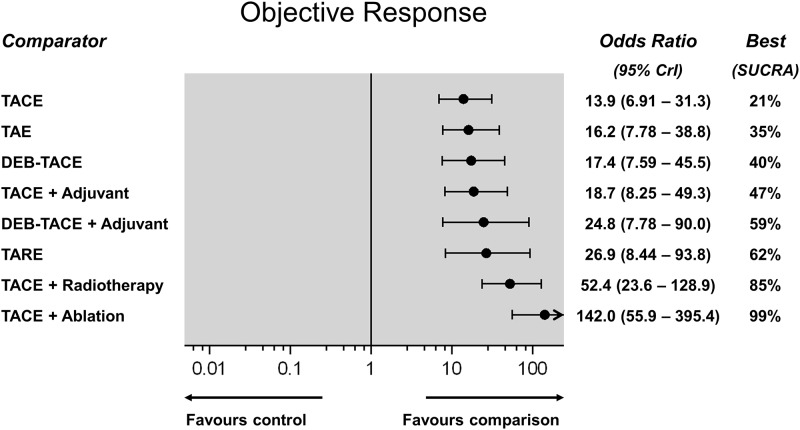
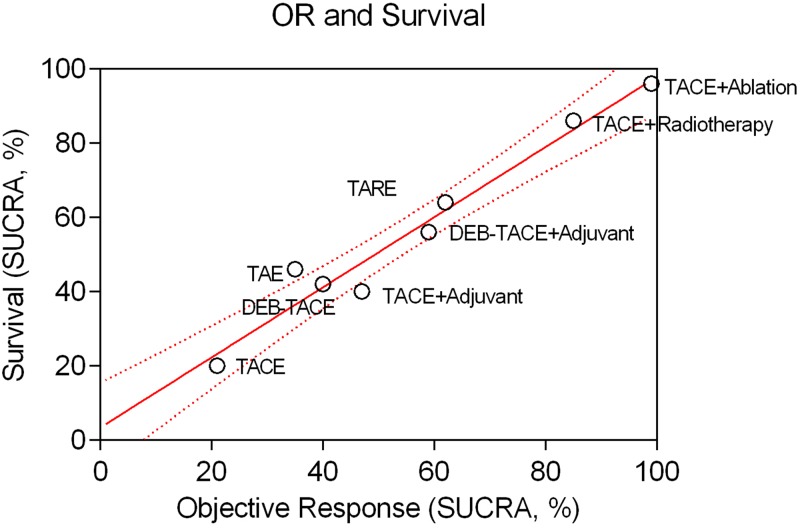
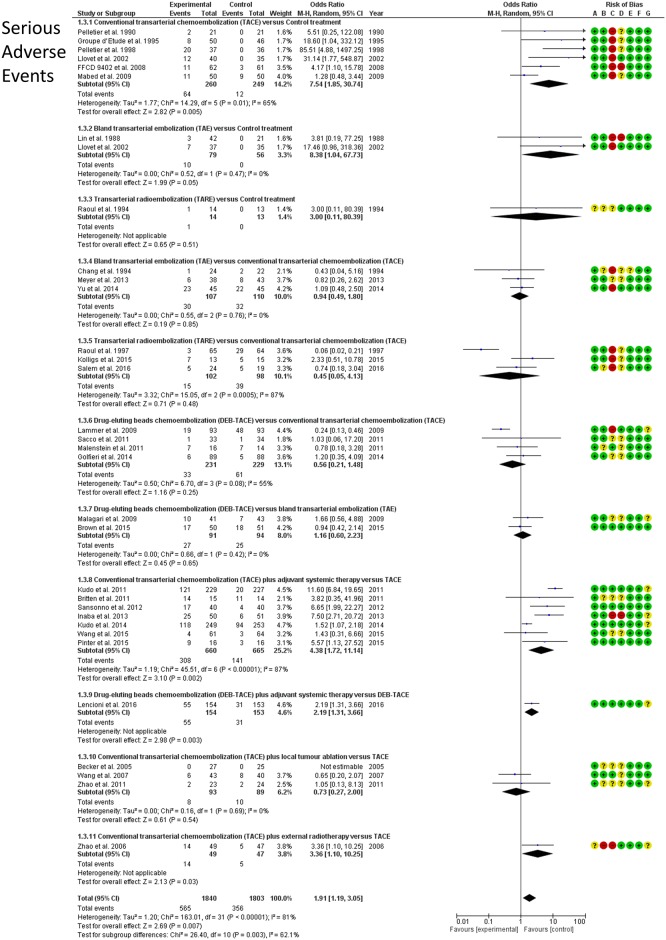
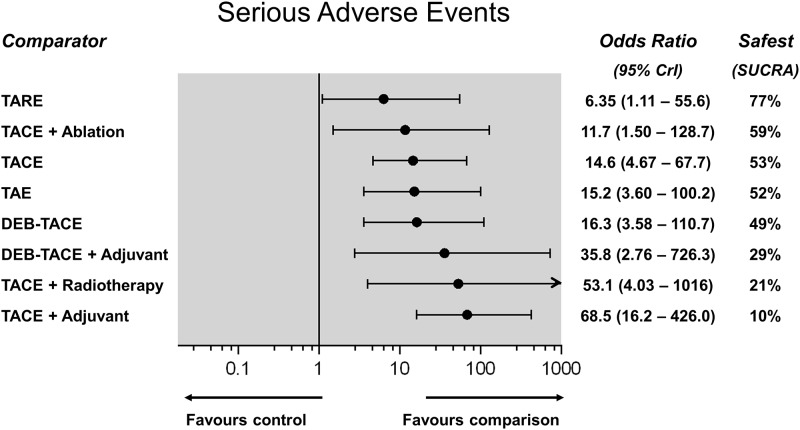
Findings: The network of evidence included 55 RCTs (12 direct comparisons) with 5,763 patients with preserved liver function and unresectable HCC (intermediate to advanced stage). All embolization strategies achieved a significant survival gain over control treatment (HR range, 0.42-0.76; very low-to-moderate QoE). However, TACE, DEB-TACE, TARE and adjuvant systemic agents did not confer any survival benefit over bland TAE alone (moderate QoE, except low in case of TARE). There was moderate QoE that TACE combined with external radiation or liver ablation achieved the best patient survival (SUCRA 86% and 96%, respectively). Estimated median survival was 13.9 months in control, 18.1 months in TACE, 20.6 months with DEB-TACE, 20.8 months with bland TAE, 30.1 months in TACE plus external radiotherapy, and 33.3 months in TACE plus liver ablation. TARE was the safest treatment (SUCRA 77%), however, all examined therapies were associated with a significantly higher risk of toxicity over control (OR range, 6.35 to 68.5). TACE, DEB-TACE, TARE and adjuvant systemic agents did not improve objective response over bland embolization alone (OR range, 0.85 to 1.65). There was clinical diversity among included randomized controlled trials, but statistical heterogeneity was low.
Conclusions: Chemo- and radio-embolization for unresectable hepatocellular carcinoma may improve tumour objective response and patient survival, but are not more effective than bland particle embolization. Chemoembolization combined with external radiotherapy or local liver ablation may significantly improve tumour response and patient survival rates over embolization monotherapies. Quality of evidence remains mostly low to moderate because of clinical diversity.
Systematic review registration: CRD42016035796 (http://www.crd.york.ac.uk/PROSPERO).
Conflict of interest statement
Figures
Similar articles
-
Ablative and non-surgical therapies for early and very early hepatocellular carcinoma: a systematic review and network meta-analysis.Health Technol Assess. 2023 Dec;27(29):1-172. doi: 10.3310/GK5221. Health Technol Assess. 2023. PMID: 38149643 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Management of people with early- or very early-stage hepatocellular carcinoma: an attempted network meta-analysis.Cochrane Database Syst Rev. 2017 Mar 28;3(3):CD011650. doi: 10.1002/14651858.CD011650.pub2. Cochrane Database Syst Rev. 2017. PMID: 28351116 Free PMC article.
-
External beam radiotherapy for unresectable hepatocellular carcinoma.Cochrane Database Syst Rev. 2017 Mar 7;3(3):CD011314. doi: 10.1002/14651858.CD011314.pub2. Cochrane Database Syst Rev. 2017. PMID: 28267205 Free PMC article.
Cited by
-
A scoring model combining serum alpha-fetoprotein and tumor size and number predicts prognosis in hepatitis B virus-related hepatocellular carcinoma patients after curative hepatectomy.Transl Cancer Res. 2019 Aug;8(4):1438-1448. doi: 10.21037/tcr.2019.07.49. Transl Cancer Res. 2019. PMID: 35116886 Free PMC article.
-
Transarterial chemoembolization for hepatocellular carcinoma: 2023 expert consensus-based practical recommendations of the Korean Liver Cancer Association.J Liver Cancer. 2023 Sep;23(2):241-261. doi: 10.17998/jlc.2023.05.22. Epub 2023 Jul 14. J Liver Cancer. 2023. PMID: 37449302 Free PMC article.
-
Sarcopenia as a predictor of survival in patients undergoing bland transarterial embolization for unresectable hepatocellular carcinoma.PLoS One. 2020 Jun 17;15(6):e0232371. doi: 10.1371/journal.pone.0232371. eCollection 2020. PLoS One. 2020. PMID: 32555707 Free PMC article.
-
Comparison of Trans-Arterial Chemoembolization and Bland Embolization for the Treatment of Hepatocellular Carcinoma: A Propensity Score Analysis.Cancers (Basel). 2021 Feb 15;13(4):812. doi: 10.3390/cancers13040812. Cancers (Basel). 2021. PMID: 33672012 Free PMC article.
-
Identification of a Pyroptosis-Related Gene Signature for Predicting Overall Survival and Response to Immunotherapy in Hepatocellular Carcinoma.Front Genet. 2021 Dec 3;12:789296. doi: 10.3389/fgene.2021.789296. eCollection 2021. Front Genet. 2021. PMID: 34925465 Free PMC article.
References
-
- Bruix J, Sherman M, Practice Guidelines Committee AAftSoLD. Management of hepatocellular carcinoma. Hepatology. 2005;42(5):1208–36. doi: 10.1002/hep.20933 . - DOI - PubMed
-
- de Baere T, Arai Y, Lencioni R, Geschwind JF, Rilling W, Salem R, et al. Treatment of Liver Tumors with Lipiodol TACE: Technical Recommendations from Experts Opinion. Cardiovasc Intervent Radiol. 2016;39(3):334–43. doi: 10.1007/s00270-015-1208-y . - DOI - PubMed
-
- Llovet JM, Zucman-Rossi J, Pikarsky E, Sangro B, Schwartz M, Sherman M, et al. Hepatocellular carcinoma. Nature reviews Disease primers. 2016;2:16018 doi: 10.1038/nrdp.2016.18 . - DOI - PubMed
-
- Bruix J, Reig M, Sherman M. Evidence-Based Diagnosis, Staging, and Treatment of Patients With Hepatocellular Carcinoma. Gastroenterology. 2016;150(4):835–53. doi: 10.1053/j.gastro.2015.12.041 . - DOI - PubMed
-
- Mathurin P, Rixe O, Carbonell N, Bernard B, Cluzel P, Bellin MF, et al. Review article: Overview of medical treatments in unresectable hepatocellular carcinoma—an impossible meta-analysis? Alimentary pharmacology & therapeutics. 1998;12(2):111–26. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
