

Household costs and time to seek care for pregnancy related complications: The role of results-based financing
- PMID: 28934320
- PMCID: PMC5608189
- DOI: 10.1371/journal.pone.0182326
Household costs and time to seek care for pregnancy related complications: The role of results-based financing
Abstract
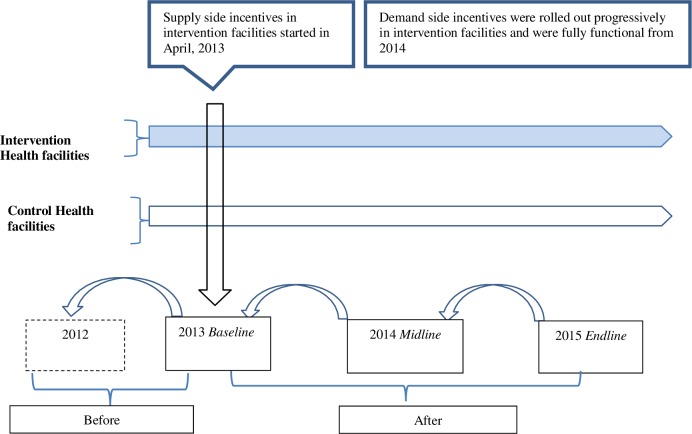
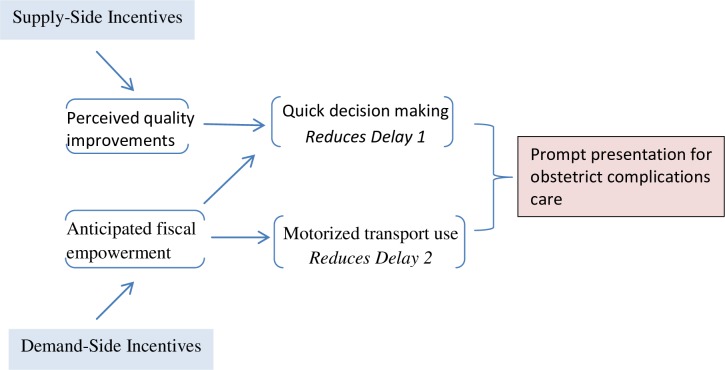
Results-based financing (RBF) schemes-including performance based financing (PBF) and conditional cash transfers (CCT)-are increasingly being used to encourage use and improve quality of institutional health care for pregnant women in order to reduce maternal and neonatal mortality in low-income countries. While there is emerging evidence that RBF can increase service use and quality, little is known on the impact of RBF on costs and time to seek care for obstetric complications, although the two represent important dimensions of access. We conducted this study to fill the existing gap in knowledge by investigating the impact of RBF (PBF+CCT) on household costs and time to seek care for obstetric complications in four districts in Malawi. The analysis included data on 2,219 women with obstetric complications from three waves of a population-based survey conducted at baseline in 2013 and repeated in 2014(midline) and 2015(endline). Using a before and after approach with controls, we applied generalized linear models to study the association between RBF and household costs and time to seek care. Results indicated that receipt of RBF was associated with a significant reduction in the expected mean time to seek care for women experiencing an obstetric complication. Relative to non-RBF, time to seek care in RBF areas decreased by 27.3% (95%CI: 28.4-25.9) at midline and 34.2% (95%CI: 37.8-30.4) at endline. No substantial change in household costs was observed. We conclude that the reduced time to seek care is a manifestation of RBF induced quality improvements, prompting faster decisions on care seeking at household level. Our results suggest RBF may contribute to timely emergency care seeking and thus ultimately reduce maternal and neonatal mortality in beneficiary populations.
Conflict of interest statement
Figures
References
-
- Orenstein LA, Orenstein EW, Teguete I, Kodio M, Tapia M, Sow SO, et al. Background rates of adverse pregnancy outcomes for assessing the safety of maternal vaccine trials in sub-Saharan Africa. PLoS One. 2012;7(10):e46638 Epub 2012/10/12. doi: 10.1371/journal.pone.0046638 ; PubMed Central PMCID: PMCPmc3464282. - DOI - PMC - PubMed
-
- Maine D. Safe motherhood progress, options and issues New York, NY: Columbia University Center for Population and Family Health; 1991.
-
- Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38(8):1091–110. Epub 1994/04/01. . - PubMed
-
- Campbell MR, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. The Lancet. 2006;368(9543):1284–99. doi: https://doi.org/10.1016/S0140-6736(06)69381-1 - DOI - PubMed
-
- Hussein J, Kanguru L, Astin M, Munjanja S. The effectiveness of emergency obstetric referral interventions in developing country settings: a systematic review. PLoS Med. 2012;9(7):e1001264 Epub 2012/07/19. doi: 10.1371/journal.pmed.1001264 ; PubMed Central PMCID: PMCPmc3393680. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
