

High Early Fluid Input After Aneurysmal Subarachnoid Hemorrhage: Combined Report of Association With Delayed Cerebral Ischemia and Feasibility of Cardiac Output-Guided Fluid Restriction
- PMID: 28934895
- PMCID: PMC6927070
- DOI: 10.1177/0885066617732747
High Early Fluid Input After Aneurysmal Subarachnoid Hemorrhage: Combined Report of Association With Delayed Cerebral Ischemia and Feasibility of Cardiac Output-Guided Fluid Restriction
Abstract
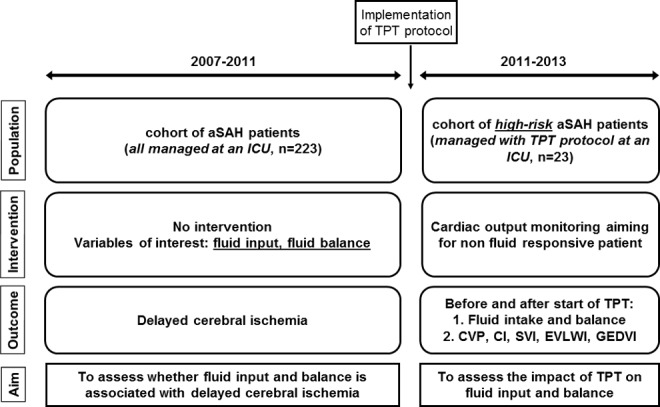
Background: Guidelines on the management of aneurysmal subarachnoid hemorrhage (aSAH) recommend euvolemia, whereas hypervolemia may cause harm. We investigated whether high early fluid input is associated with delayed cerebral ischemia (DCI), and if fluid input can be safely decreased using transpulmonary thermodilution (TPT).
Methods: We retrospectively included aSAH patients treated at an academic intensive care unit (2007-2011; cohort 1) or managed with TPT (2011-2013; cohort 2). Local guidelines recommended fluid input of 3 L daily. More fluids were administered when daily fluid balance fell below +500 mL. In cohort 2, fluid input in high-risk patients was guided by cardiac output measured by TPT per a strict protocol. Associations of fluid input and balance with DCI were analyzed with multivariable logistic regression (cohort 1), and changes in hemodynamic indices after institution of TPT assessed with linear mixed models (cohort 2).
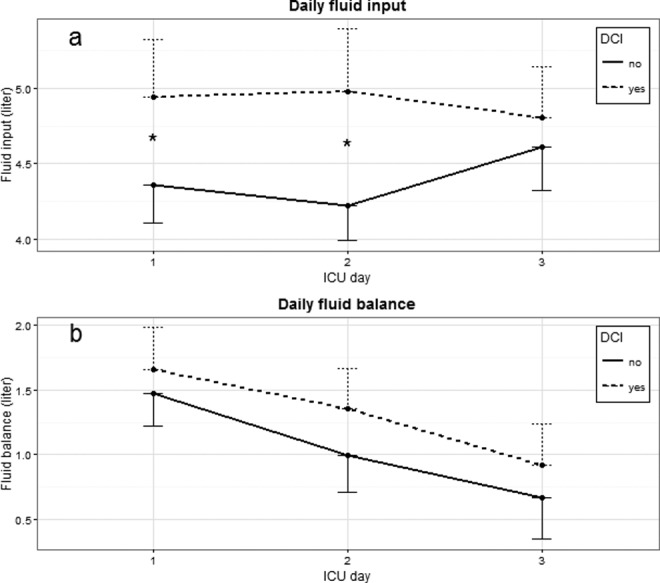
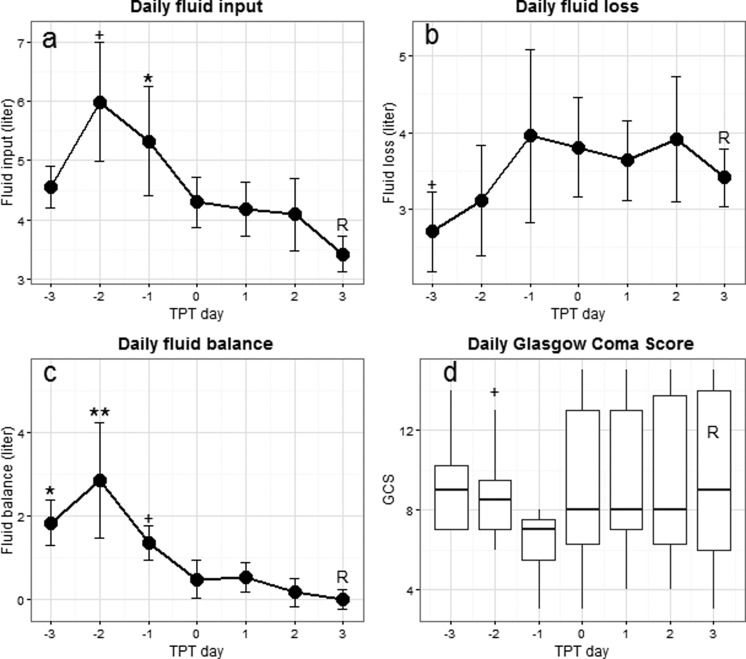
Results: Cumulative fluid input 0 to 72 hours after admission was associated with DCI in cohort 1 (n=223; odds ratio [OR] 1.19/L; 95% confidence interval 1.07-1.32), whereas cumulative fluid balance was not. In cohort 2 (23 patients), using TPT fluid input could be decreased from 6.0 ± 1.0 L before to 3.4 ± 0.3 L; P = .012), while preload parameters and consciousness remained stable.
Conclusion: High early fluid input was associated with DCI. Invasive hemodynamic monitoring was feasible to reduce fluid input while maintaining preload. These results indicate that fluid loading beyond a normal preload occurs, may increase DCI risk, and can be minimized with TPT.
Keywords: aneurysmal subarachnoid hemorrhage; delayed cerebral ischemia; fluid management; hypervolemia; transpulmonary thermodilution.
Conflict of interest statement
Figures
References
-
- Vergouwen MD; Participants in the International Multi-Disciplinary Consensus Conference on the Critical Care Management of Subarachnoid Hemorrhage. Vasospasm versus delayed cerebral ischemia as an outcome event in clinical trials and observational studies. Neurocrit Care. 2011;15(2):308–311. - PubMed
-
- van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007;369(9558):306–318. - PubMed
-
- Vergouwen MD, Ilodigwe D, Macdonald RL. Cerebral infarction after subarachnoid hemorrhage contributes to poor outcome by vasospasm-dependent and -independent effects. Stroke. 2011;42(4):924–929. - PubMed
-
- Connolly ES, Jr, Rabinstein AA, Carhuapoma JR, et al. American Heart Association Stroke C, Council on Cardiovascular R, Intervention, Council on Cardiovascular N, Council on Cardiovascular S, Anesthesia, Council on Clinical C. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2012;43(6):1711–1737. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
