

Treatment and outcomes of tumor-induced osteomalacia associated with phosphaturic mesenchymal tumors: retrospective review of 12 patients
- PMID: 28934935
- PMCID: PMC5609032
- DOI: 10.1186/s12891-017-1756-1
Treatment and outcomes of tumor-induced osteomalacia associated with phosphaturic mesenchymal tumors: retrospective review of 12 patients
Abstract
Background: Tumor-induced osteomalacia (TIO) is a rare paraneoplastic syndrome characterized by severe hypophosphatemia and osteomalacia. Nonspecific symptoms make the diagnosis elusive. In addition, locating the responsible tumor(s) is challenging. The aim of this study was to investigate the clinical management and outcomes of TIO.
Methods: The clinical features, diagnostic procedures, treatment, and outcomes of 12 patients were reviewed retrospectively.
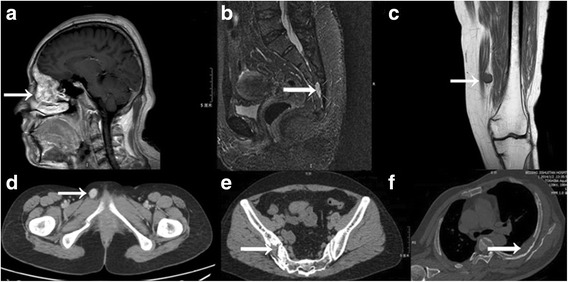
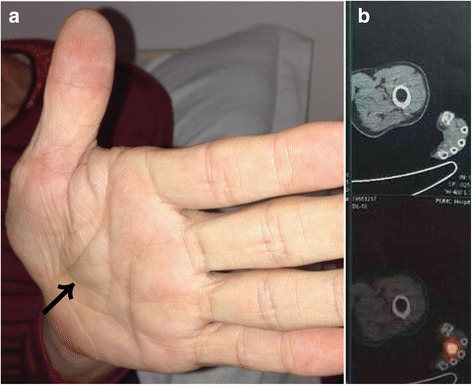
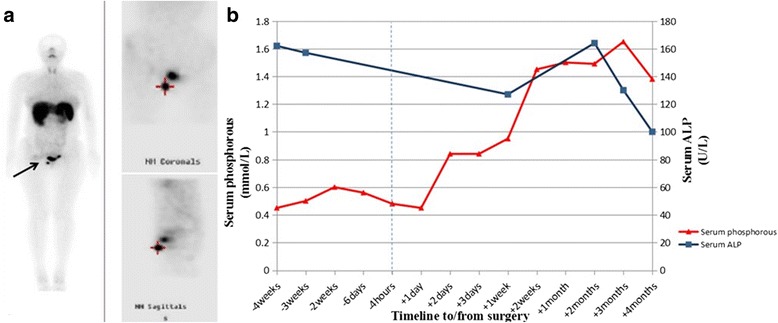
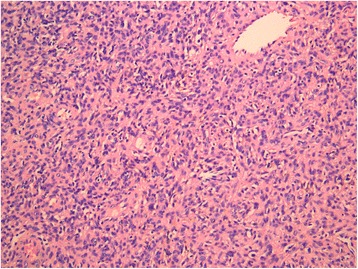
Results: The cohort comprised six men and six women (mean age 45.5 ± 9.9 years, range 23-61 years). The mean duration of disease was 3.7 ± 2.6 years. All patients manifested progressive bone pain, muscle weakness, and/or difficulty walking. Serum phosphorus concentrations were low in all patients (mean 0.42 ± 0.12 mmol/L). Technetium-99m octreotide scintigraphy was performed in 11 patients and showed lesions in the right distal femur, left femoral head, and right tibial plateau, respectively, in three patients. Magnetic resonance imaging (MRI) was negative for lesions in one patient. Two patients underwent biopsies that showed negative histopathology. Two patients, at 2 years and 8 months, respectively, after having negative technetium-99m octreotide studies, underwent 18F-fluorodeoxyglucose positron emission tomography/computed tomography (CT), which revealed lesions in the sacrum and soft tissue of the left palm, respectively. One tumor was detected by CT and MRI. Overall, lesion sites were the head (two patients, 16.7%), thoracic and lumbar region (two, 16.7%), pelvis (three, 25%), lower limbs (four, 33.3%), and upper limbs (one, 8.3%). All patients underwent surgery, and histopathology showed phosphaturic mesenchymal tumors in each. Postoperatively, serum phosphorus concentrations normalized within 2-7 days in 11 patients. With follow-ups of 1-41 months, surgery was effective in 10 patients. One patient developed local recurrence and another had metastases.
Conclusions: Locating tumors responsible for tumor-induced osteomalacia is often challenging. Although complete tumor resection confers a good prognosis in most patients, surveillance for recurrence and metastasis is necessary. Before surgery or when surgery is not indicated, oral phosphate can alleviate symptoms and metabolic imbalance.
Keywords: Fibroblast growth factor 23; Fractures; Hypophosphatemia; Oncogenic osteomalacia; Phosphaturic mesenchymal tumor; Spontaneous.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by Beijing Jishuitan Hospital Institutional Review Board (committee reference number 201608–02). Written informed consent was obtained from all participants before they participated in the study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ward LM, Rauch F, White KE, Filler G, Matzinger MA, Letts M, Travers R, Econs MJ, Glorieux FH. Resolution of severe, adolescent-onset hypophosphatemic rickets following resection of an FGF-23-producing tumour of the distal ulna. Bone. 2004;34(5):905–911. doi: 10.1016/j.bone.2003.12.025. - DOI - PubMed
-
- Jiang Y, Xia WB, Xing XP, Silva BC, Li M, Wang O, Zhang HB, Li F, Jing HL, Zhong DR, et al. Tumor-induced osteomalacia: an important cause of adult-onset hypophosphatemic osteomalacia in China: Report of 39 cases and review of the literature. J Bone Miner Res. 2012;27(9):1967–1975. doi: 10.1002/jbmr.1642. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
